


Translate this page into:
Cytodiagnosis of gouty tophus
-
Received: ,
Accepted: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
To the Editor,
Periarticular nodule can prove to be a challenge to both clinicians and pathologists. It covers inflammatory to neoplastic conditions ranging from rheumatoid nodule, gout, giant cell tumor of tendon sheath, synovial osteochondromatosis to synovial sarcoma.[1] Amongst these, gouty tophus is an important differential. Fine Needle Aspiration Cytology (FNAC) is becoming popular in diagnosis of soft tissue nodules; hence it is important for the pathologists to be aware of its varied microscopic features. Here, we present clinical and cytological profile of a case of gouty tophus.[12]
A 62 year male presented with swelling over left middle toe of 6 months duration. It was painful and gradually increasing in size. On examination it measured 2 cm × 1 cm, immobile, firm to hard, tender with tense overlying skin [Figure 1]. Patient gave a past history of nephrolithiasis about 8 years back for which he was treated. On investigations, his Erythrocyte sedimentation rate (ESR) was 36 mm at the end of 1 h. His hemogram, liver function tests, serum calcium level and rheumatoid factor were within the normal limits. Blood urea was 98 mg/dl, serum creatinine 3.1 mg/dl and serum uric acid 9.1 mg/dl. Radiograph of the lesion showed a soft-tissue swelling without involvement of underlying bone with no evidence of calcification. FNA from the swelling, yielded whitish, and granular material. Smears prepared were wet fixed in 95% ethanol and some were also air dried. The wet fixed smears were stained with H and E and Papanicolaou stains. The air dried smears were stained with May Grunwald Giemsa stain (MGG). Smears revealed amorphous crystalline material intermingled with which were few histiocytes and foreign body giant cells [Figure 2]. The crystalline material on the higher magnification particularly with MGG revealed elongated needle shaped crystals with pointed ends [Figure 3]. The diagnosis of gouty tophus was made on the cytology, which was further supported by elevated levels of serum uric acid. Smears were not examined under polarized microscope as this facility was unavailable. Being a medically treatable condition, excision of the mass was not done and the clinicians directly put the patient on the anti-uric acid drugs.

- Nodular swelling 2 × 1 × 1 cm in size, firm, immobile, non-tender, with tense overlying skin
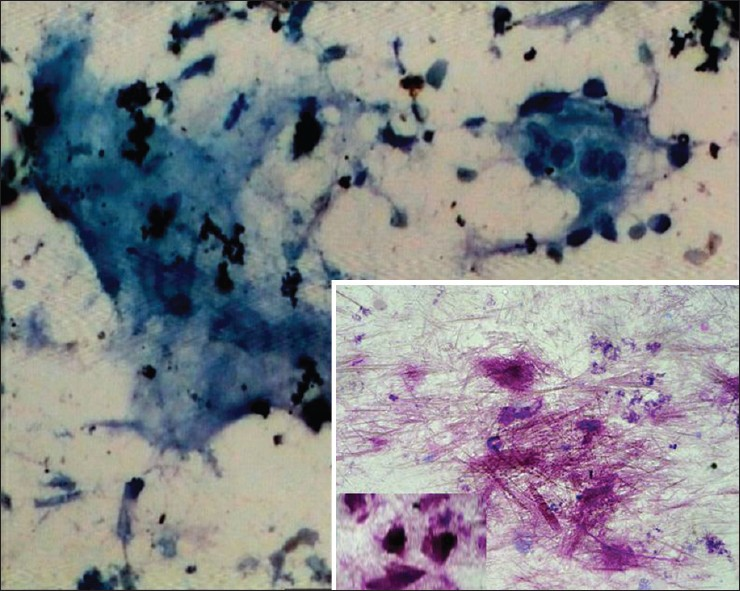
- Amorphous granular material and foreign body giant cell (Papanicolaou ×20) (Inset showing elongated crystals MGG x20)
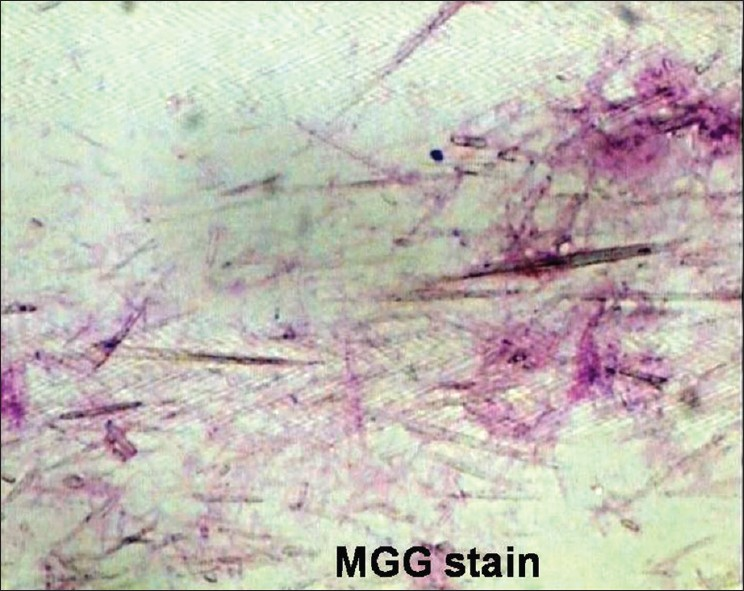
- Elongated needle shaped crystals with pointed tips (MGG × 40)
FNAC is an easy alternative to synovial biopsy and joint fluid analysis in a case of gouty tophus.[3] Whenever an aspiration yields amorphous or granular material, the cytopathologists should carefully search for characteristic crystals especially in MGG. Although gouty tophus presents classic histological features, definitive diagnosis relies on the demonstration of crystals which are often dissolved in routine tissue processing.[3] However, these crystals are excellently preserved and demonstrated in air dried smears stained with MGG. These monosodium urate crystals are needle shaped rods about 5-20 u in length with pointed tips. They are also strongly birefringent.[4] On histology, gouty tophus shows large amorphous aggregates of urate crystals surrounded by intense inflammatory cells macrophages, lymphocytes, foreign body giant cells, and fibroblastic reaction. However, the morphology of individual crystals cannot be appreciated well. The tissue diagnosis can be of additional help to demonstrate birefringence if this ancillary technique is available.[56]
FNAC offers a simple, cost effective tool in elucidating the nature of periarticular nodule.[134] In case of gouty tophus, it also has an added advantage of excellent preservation of crystals. Thus, if a pathologist is aware of its morphology, further unnecessary investigations can be avoided. Patient was subsequently puts on the antiuric acid drugs. After a period of 3 months, swelling reduced remarkably in size and uric acid level decreased to 4.6 mg/dl.
COMPETING INTERESTS STATEMENT BY ALL AUTHORS
The authors declare that they have no competing interests.
AUTHORSHIP STATEMENT BY ALL AUTHORS
All authors of this article declare that they qualify for authorship as defined by ICMJE. All authors participated in its design and coordination, and worked collaboratively to draft the manuscript. All authors read and approved the final manuscript.
ETHICS STATEMENT BY ALL AUTHORS
This manuscript is a case description in form of a letter. Therefore IRB approval was not mandatory by our institution.
EDITORIAL/PEER-REVIEW STATEMENT
To ensure the integrity and highest quality of CytoJournal publications, the review process of this manuscript was conducted under a double blind model (authors are blinded for reviewers and vice versa) through automatic online system
Available FREE in open access from: http://www.cytojournal.com/text.asp?2013/10/1/11/112649
REFERENCES
- Fine needle aspiration cytology of gouty tophy with review of literature. J Cytol. 2007;24:142-5.
- [Google Scholar]
- Diagnostic value of fine needle aspiration cytology in gouty tophi: A report of 7 cases. Acta Cytol. 2006;50:101-4.
- [Google Scholar]
- Staining method to demonstrate urate crystals in formalin-fixed, paraffin-embedded tissue sections. Arch Pathol Lab Med. 2000;124:774-6.
- [Google Scholar]
- Evaluation of crystals in formalin-fixed, paraffin-embedded tissue sections for the differential diagnosis of pseudogout, gout, and tumoral calcinosis. Mod Pathol. 2001;14:806-10.
- [Google Scholar]




