


Translate this page into:
Cytological diagnosis of osteoblastoma of the talus: Case report with unusual presentation and diagnostic pitfalls
-
Received: ,
Accepted: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Osteoblastoma is a rare bone tumor mostly affecting the young adults and commonly involving the spinal cord and long bones. Talus is the uncommon site of presentation, and if involved, then the neck is more commonly involved than the body of talus. The cytological diagnosis of osteoblastoma is limited, and to the best of our knowledge, its fine-needle aspiration (FNA) in the talus has still not been reported in the literature. The present case of osteoblastoma is, therefore, being reported due to the unusual presentation in elderly male in the body of talus and showing extensive involvement on X-ray. The case was initially diagnosed on FNA cytology excluding the possibility of giant-cell tumor and osteosarcoma. The case also highlights the importance of vigilant observation of subtle cytological features of this rare tumor which may be helpful in avoiding diagnostic pitfalls, especially at an uncommon site and with unusual presentation. An early precise diagnosis by cytology may be followed by appropriate treatment and thus avoiding any further complications.
Keywords
Diagnostic pitfalls
fine-needle aspiration cytology
osteoblastoma
talus

INTRODUCTION
Osteoblastoma is a rare tumor which accounts to 1% of all bone tumors with male preponderance and mostly affecting the teenagers or young adults.[12] The tumor commonly presents in spine, sacrum, tibia, and fibula, while bones of hand, foot, ribs, and scapula are considered to be the uncommon sites of presentation.[34] Moreover, if talus is involved, then neck is the usual site of presentation while body of the talus is rarely involved.[56] The cytological diagnosis of osteoblastoma is limited and only few single cases have been reported in the literature while fine-needle aspiration cytology (FNAC) of osteoblastoma in talus has still not been reported.[7] The present case of osteoblastoma is, therefore, being reported which presented in elderly male in the body of talus with extensive involvement and initially diagnosed on cytopathology. The case lays the importance of close examination of subtle cytological features of this rare tumor so that diagnostic pitfalls may be avoided, especially if presenting at an uncommon site with unusual presentation.
CASE REPORT
A 50-year-old male presented with the swelling over left ankle for the past 2 years with a history of trauma. The swelling was large (10 cm × 5 cm × 5 cm), fluctuant, progressively increasing in size, and associated with pain [Figure 1a]. His X-ray left ankle revealed expansile osteolytic destruction of the body of talus extending to the lower end of tibia and fibula with soft tissue involvement [Figure 1b], and clinical differential diagnosis of giant-cell tumor (GCT) or osteosarcoma was considered. The patient was subjected to FNAC which showed cellular smears with the presence of mononuclear and binucleated osteoblasts along with scattered osteoclastic giant cells and uniform spindle cells entangled in myxoid stroma [Figure 2a–d]. No necrosis and no atypical mitosis were observed. In view of mostly uniform osteoblasts with the absence of necrosis and no atypical mitosis, the possibility of osteosarcoma (osteoblastic variant) was excluded. Close examination of smears also excluded GCT as there were scattered osteoclastic giant cells without any definite arrangement, fair number of osteoblasts, and no mononuclear cells. The final diagnosis of benign osteoblastoma was given on cytology. In view of the large lesion, surgical excision was performed and subsequent histopathology confirmed the diagnosis of osteoblastoma [Figure 2e and f]. The patient responded well to the treatment without any history of recurrence and is on constant follow-up.
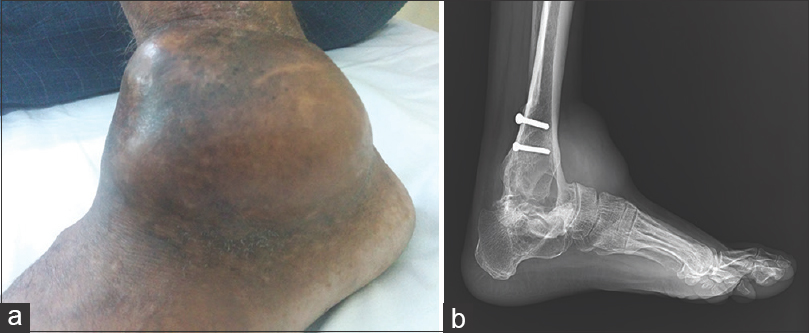
- (a) Large swelling in the left ankle. (b) X-ray left ankle revealed expansile osteolytic destruction of the body of talus extending to lower end of tibia and fibula with soft tissue involvement
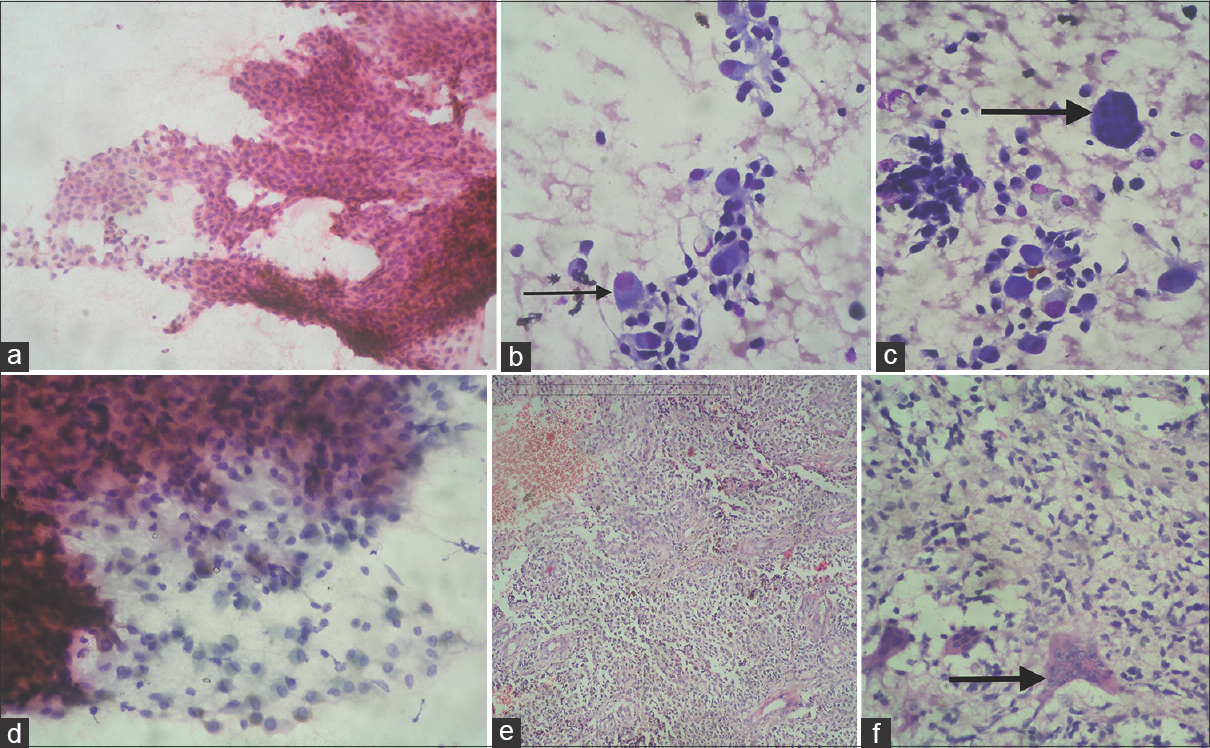
- (a-d) Fine-needle aspiration cytology of the swelling showed cellular tumor with osteoblasts (thin arrow), scattered giant cells (thick arrow), and spindle cells entangled in myxoid matrix (May-Grunwald-Giemsa, ×40; H and E, ×40). (e and f) Histopathological examination showed cellular osteoblastic tumor with ectatic blood vessels and scattered giant cells (thick arrow) (H and E, ×40)
DISCUSSION
Osteoblastoma is a rare benign tumor of the bone commonly seen in young adults in the second and third decades of life, and it is reported that 90% of cases are diagnosed before the age of 30.[4] Long tubular bones and spine are although considered to be a common site of the tumor, less commonly, it may involve bones of hand, feet, maxilla, and ileum.[189] Gupta et al. observed a single case of osteoblastoma on FNAC of 158 lesions of nose, nasal cavity, and paranasal sinuses.[10] Talus is the unusual site of presentation, and neck of the talus is more commonly involved than the body of talus.[5611] The case which is being reported presented with unusual presentation of osteoblastoma in body of talus in an elderly male of 50 years. The tumor was expansile on X-ray and also involved the lower end of tibia and fibula with soft tissue involvement, and clinical differential diagnosis of the aggressive tumor including GCT or osteosarcoma was considered. The X-ray examination of the osteoblastoma is nonspecific, and mostly, the lesion is well circumscribed and partially calcified while aggressive osteoblastoma may show moth-eaten permeated appearance.[12] Osteoblastic osteosarcoma which is an important differential diagnosis of osteoblastoma differs radiologically by usually presenting in the subperiosteal region and arising in metaphysis or diaphysis comprising the lytic and sclerotic component with cortical disruption while osteoblastoma occurs in cortical or medullary bone.[13] The case was subjected to FNAC and diagnosis of benign osteoblastoma was given which was later confirmed on histopathology. The cytological diagnosis of osteoblastoma is limited and confined to few single cases presenting in spine or ileum, and to the best of our knowledge, FNAC of the talus has still not been reported in the literature.[39] This is especially important as differential diagnosis include other common tumors of this site, and careful examination of cytomorphological features is important to avoid diagnostic pitfalls. In addition, delayed diagnosis of aggressive osteoblastoma may be associated with recurrence, malignant transformation, or distant metastasis of this tumor.[14] Therefore, cytology may be an important diagnostic tool in early diagnosis of osteoblastoma. The typical osteoblastoma on FNAC will show osteoblasts with mild pleomorphism along with tight clusters of uniform spindle cells entangled in the myxoid matrix and few scattered osteoclastic giant cells. Atypical mitotic figures and necrosis are absent [Figure 2]. GCT is considered to be an important differential diagnosis, and features which may be helpful in avoiding diagnostic pitfalls are the presence of spindle cells clusters showing the peripheral arrangement of a fair number of osteoclastic giant cells, resulting in a checkerboard pattern in GCT. In contrast, osteoblastoma will show few scattered osteoclastic giant cells without any definite arrangement. In addition, typical osteoblasts with perinuclear hof are absent in GCT which instead shows mononuclear round cells with central uniform nuclei [Figure 3]. Another important differential diagnosis of osteoblastoma is osteoblastic osteosarcoma, especially if osteoblastoma is aggressive. The important clue which may be helpful in clinching the diagnosis of osteoblastoma even if it is aggressive is that osteoblasts may show pleomorphism, but nuclear chromatin is mostly uniform with perinuclear hof. In addition, frequent atypical mitosis and osteoid matrix within cell clusters are not appreciated in osteoblastoma [Figure 4]. Sathiyamoorthy et al. reviewed 22 cases of osteoblastic osteosarcoma with most of the cases presenting in long bones.[13] They observed that cytologically, osteoblastic osteosarcoma shows cellular smears with discohesive single cells, immature osteoid, osteoclastic giant cells, plasmacytoid cells with basophilic vacuolated cytoplasm, round nuclei, and macronucleoli. In addition, they also observed severe pleomorphism, numerous mitotic figures, and high-grade cytologic atypia in 10 cases of osteoblastic osteosarcoma.[13] FNAC of osteoblastoma usually lacks the above-mentioned cytological features and this may be helpful in avoiding the diagnostic pitfall. Rhode et al. have reported a single case of osteoblastoma on FNAC presenting in the spinal cord and associated with lymphangiomatosis.[15] They have suggested that FNA is favorable to radiography and could be valuable in the diagnostic workup of bone tumors when clinical or radiological parameters do not agree.[1516] The present case also supports the importance of FNAC in the diagnosis of this rare benign tumor as clinicoradiologically it presented as an aggressive tumor. It has been reported that genetic alterations are low in osteoblastoma in comparison to osteosarcoma, and murine double minute 2 amplification and TP53 deletion correlate with the aggressive potential of osteoblastoma.[1] It has also been reported that immunochemical expression of cyclooxygenase-2 may be helpful in differentiating low-grade osteosarcoma and aggressive osteoblastoma which is negative in osteosarcoma.[17]
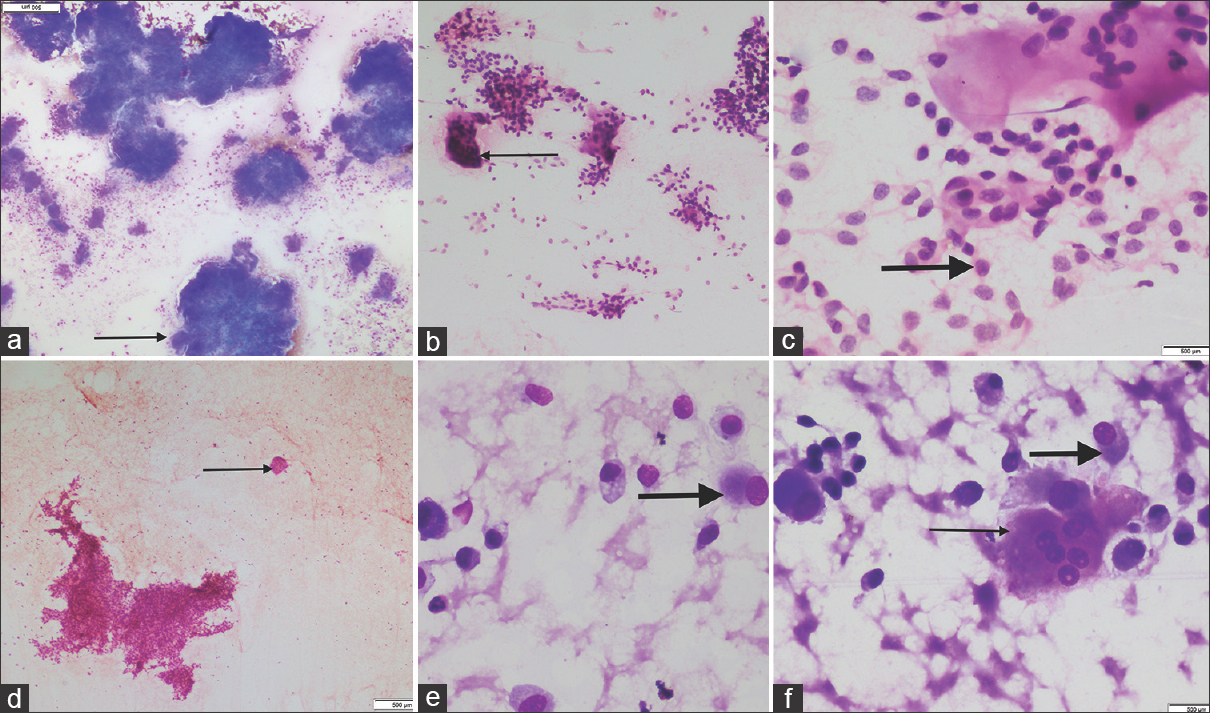
- (a-c) Fine-needle aspiration cytology of giant-cell tumor showed spindle cell clusters and numerous osteoclasts arranged at the periphery of the clusters with checkerboard pattern (thin arrow). The mononuclear round cells show central uniform nuclei (thick arrow) (May-Grunwald-Giemsa, ×4; H and E, ×10 and ×40) (This figure of giant-cell tumor is original and is from another case. It is shown for comparison with osteoblastoma and has no relation with present case). (d-f) In contrast, fine-needle aspiration cytology of osteoblastoma showed few scattered osteoclastic giant cells (thin arrow) with fair number of osteoblasts having perinuclear hof (thick arrow) (May-Grunwald-Giemsa, ×40; H and E, ×4)
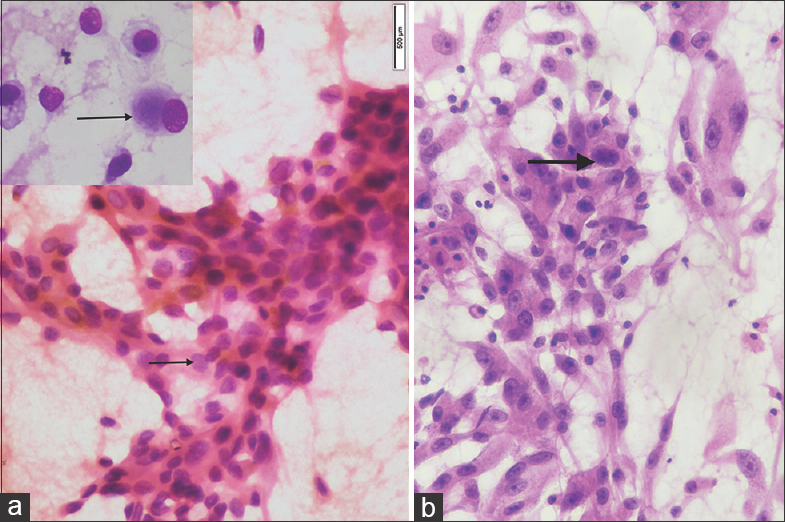
- (a) Fine-needle aspiration cytology of osteoblastoma showed osteoblasts with perinuclear hof (inset) and cells showing uniform fine chromatin with inconspicuous nucleoli (thin arrow). Atypical mitosis is not seen (May-Grunwald-Giemsa, ×40; H and E, ×40). (b) Fine-needle aspiration cytology of osteosarcoma showed cellular smears comprising round-to-spindle cells with moderate-to-severe pleomorphism and nucleus with coarse chromatin and prominent nucleoli (thick arrow). Mitotic figures are present (H and E, ×40) (This figure of osteosarcoma is original and is from another case. It is shown for comparison with osteoblastoma and has no relation with the present case)
The treatment strategy of osteoblastoma includes curettage or excision with good prognosis. However, aggressive osteoblastoma may need radiotherapy or chemotherapy to prevent recurrence or metastasis. The present case underwent excision as it was large and the patient responded well without any recurrence.
Thus, to summarize, the present case highlights the unusual presentation of a rare tumor, osteoblastoma of the body of the talus in an elderly male. The case also lays the importance of FNAC with radiological correlation in precise diagnosis of this tumor. In addition, it emphasizes the value of vigilant examination of cytological smears to identify the subtle features which may be helpful in avoiding diagnostic pitfalls. An early diagnosis by cytology may be followed by appropriate treatment and thus avoiding any further complications.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
COMPETING INTERESTS STATEMENT BY ALL AUTHORS
All authors declare that they have no competing interests.
AUTHORSHIP STATEMENT BY ALL AUTHORS
All authors have contributed significantly and agree with the final manuscript.
ETHICS STATEMENT BY ALL AUTHORS
This report does not require approval from Institutional Review Board (IRB).
LIST OF ABBREVIATIONS (In alphabetic order)
FNA - Fine-Needle Aspiration
FNAC - Fine-Needle Aspiration Cytology
GCT - Giant-Cell Tumor.
EDITORIAL/PEER-REVIEW STATEMENT
To ensure the integrity and highest quality of CytoJournal publications, the review process of this manuscript was conducted under a double-blind model (authors are blinded for reviewers and vice versa) through automatic online system.
REFERENCES
- Osteoblastoma. In: Fletcher CD, Unni KK, Mertens F, eds. WHO Classification-Tumours of Soft Tissue and Bone. Lyon: International Agency for Research on Cancer; 2002. p. :262-3.
- [Google Scholar]
- Benign osteoblastoma (giant osteoid osteoma) In: Unni KK, editor, eds. Dahlin's Bone Tumors: General Aspect and Data on 11087 Cases (5th ed). Philadelphia: Lippincott Raven; 1996. p. :131-42.
- [Google Scholar]
- Cytological diagnosis of osteoblastoma of cervical spine: A case report with review of literature. Diagn Cytopathol. 2015;43:218-21.
- [Google Scholar]
- Osteoblastoma of the sternum – Case report and review of the literature. Bull NYU Hosp Jt Dis. 2010;68:55-9.
- [Google Scholar]
- Osteoblastoma of body of the talus – Report of a rare case with atypical radiological features. Foot Ankle Surg. 2010;16:e24-6.
- [Google Scholar]
- Osteoid osteoma and osteoblastoma of the talus. A report of 40 cases. Skeletal Radiol. 1986;15:360-4.
- [Google Scholar]
- Soft tissue and musculoskeltal system. In: Winifred G, Kocjan G, eds. Diagnostic Cytopathology (3rd ed). UK: Churchill Livingstone Elsevier; 2010. p. :797-8.
- [Google Scholar]
- Benign osteoblastoma involving maxilla: A case report and review of the literature. Case Rep Dent 2012. 2012;351241
- [Google Scholar]
- Aggressive osteoblastoma of ileum: Diagnosed on FNAC. Int J Case Rep Images. 2012;3:34-8.
- [Google Scholar]
- Fine needle aspiration cytology in lesions of the nose, nasal cavity and paranasal sinuses. Acta Cytol. 2011;55:135-41.
- [Google Scholar]
- A rare case report of A young male patient presenting with osteoblastoma of the talus. J Orthop Case Rep. 2014;4:22-4.
- [Google Scholar]
- Cytological features of bone tumours in FNA smears I: Osteogenic tumours. Monogr Clin Cytol. 2010;19:18-30.
- [Google Scholar]
- Osteoblastic osteosarcoma: Cytomorphologic characteristics and differential diagnosis on fine-needle aspiration. Acta Cytol. 2012;56:481-6.
- [Google Scholar]
- Aggressive osteoblastoma with focal malignant transformation and development of pulmonary metastases. A case report with a review of literature. Gen Diagn Pathol. 1996;141:377-92.
- [Google Scholar]
- Fine-needle aspiration of spinal osteoblastoma in a patient with lymphangiomatosis. Diagn Cytopathol. 2006;34:295-7.
- [Google Scholar]
- Diagnostic accuracy and clinical utility of fine-needle aspiration cytology in the diagnosis of clinically primary bone lesions. Diagn Cytopathol. 1993;9:168-73.
- [Google Scholar]
- Role of immunohistochemical cyclo-oxygenase-2 (COX-2) and osteocalcin in differentiating between osteoblastomas and osteosarcomas. Malays J Pathol. 2012;34:15-23.
- [Google Scholar]




