


Translate this page into:
The role of intraoperative scrape cytology in vertebroplasty
-
Received: ,
Accepted: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Aims:
To assess the adequacy of intraoperative scrape cytology during percutaneous vertebroplasty by correlating results with corresponding histopathology.
Settings and Design:
Vertebroplasty is a procedure increasingly used to treat painful vertebral compression fractures. The history and presentation of osteoporotic fractures are straightforward, but difficulty arises in differentiating infective from neoplastic lesions, especially in cases where the magnetic resonance imaging is equivocal. The procedure involves injection of polymethyl methacrylate (bone cement) into the pathological vertebral body and gives dramatic pain relief. It is indicated in osteoporotic and neoplastic lesions but contraindicated in infections. Hence, intraoperative evaluation of a specimen is essential to aid in the decision of performing vertebroplasty.
Subjects and Methods:
A total of 128 patients with vertebral lesions underwent core biopsy and scrape cytology from June 2006 to June 2015. Based on the findings of cytological examination, malignant lesions were subjected to vertebroplasty. In lesions with infective etiology, vertebroplasty was abandoned and antibiotic or antituberculous therapy started.
Results:
The overall diagnostic accuracy of scrape cytology was excellent with 97.58% cases correlating with the final histopathological diagnosis. Specificity was 100%, positive predictive value was 100% and negative predictive value was 33.33%.
Conclusion:
Scrape cytology is a simple, rapid, accurate cytodiagnostic technique and should be routinely utilized in vertebral lesions for intraoperative consultation and decision making during vertebroplasty.
Keywords
Cytodiagnosis
intraoperative procedures
vertebrae
vertebroplasty

INTRODUCTION
The history of scrape cytology dates back to 1927 and its utility during intra-operative consultation has often been neglected in comparison to frozen sections and imprint cytology.[1] Scrape cytology could be preferred over touch preparation/imprint cytology as this technique yields more material. Its role as a potential tool in intraoperative consultation is more pertinent in institutions unequipped with frozen section facility.
Percutaneous transpedicular vertebroplasty is a procedure increasingly used to treat painful osteoporotic compression fractures. The history and presentation of these fractures is straightforward. Difficulty arises in differentiating infective from neoplastic lesions, especially in cases where magnetic resonance imaging (MRI) is equivocal.
Percutaneous vertebroplasty[23] is a technique wherein the vertebral body is accessed posteriorly through the pedicles. Under image intensifier control an 11–13 G bone biopsy needle (Jamshedi/Cook) is passed into the anterior 2/3 of the vertebral body. The position of the needle is verified using image intensifier. The needle is withdrawn, and the core of cancellous bone from the vertebral body sent for scrape cytology. After excluding infective pathology, the needle was passed into the vertebral body and injected with 1.5–3 ml of poly methyl methacrylate (bone cement).[4] The bone cement is fluid at the time of injection and sets into a hard mass within 10–15 min. This results in pain relief and is believed to suppress proliferation of neoplastic cells due to mass effect. Vertebroplasty is indicated in osteoporotic and metastatic lesions but contraindicated in infections.[5] Hence, intraoperative evaluation of a specimen is essential. Intraoperative scrape cytology, after transpedicular core biopsy, is a rapid and accurate cytodiagnostic tool, which can be routinely used by the orthopedic surgeon while contemplating vertebroplasty.
We report 128 patients with vertebral lesions who were subjected to transpedicular core biopsy and intraoperative scrape cytology. In this study, we emphasize the usefulness of this cytodiagnostic tool during vertebroplasty especially regarding accuracy, speed, and ease of this technique.
SUBJECTS AND METHODS
The present study was conducted between June 2006 and June 2015. One hundred twenty-eight patients with vertebral lesions where MRI findings were equivocal regarding infective or neoplastic pathology constituted the clinical material for this study. Patients with clear-cut evidence of infective etiology and patients with osteoporotic wedge compression fracture were excluded from the study. These 128 patients were referred to the pathologist for intraoperative evaluation and opinion. In all our cases we had a cytological setup adjacent to the operating theater. This was to minimize the time taken as the patient is under anesthesia. The minimum core diameter of tissue required for evaluation is between 3 and 5 mm.
Scrape technique
Using the edge of a glass slide or a clean scalpel, vertebral transpedicular core biopsy specimens were scraped [Figure 1a].

- (a) Vertebral core biopsy specimens being scraped with a scalpel. (b) Material being smeared with another glass slide
The material was smeared onto another glass slide and placed immediately while still wet in methyl alcohol [Figure 1b].
These were stained by a rapid staining procedure using hematoxylin and eosin (H and E), coverslipped and screened by the pathologist.
The time required for preparation and interpretation of a specimen by scrape preparation cytology was calculated on an average and was about 8–10 min. In addition to the diagnosis, the adequacy of the specimen was commented upon to ensure that the material was sufficient for histopathological examination. Vertebroplasty was done if the diagnosis was other than infective etiology.
The remaining tissue after completion of the cytodiagnostic technique was processed for routine paraffin section and H and E staining. The smear diagnosis was compared with the histologic diagnosis to evaluate the diagnostic accuracy.
RESULTS
The overall diagnostic accuracy of scrape cytology was excellent with 97.58% of cases correlating with the final histopathological diagnosis [Table 1]. In 128 cases, intraoperative scrape cytology was attempted. In total, 61 cases were infective lesions, with 41 cases (32%) being tuberculous etiology and 20 (15.6%) cases of pyogenic nature. The malignant lesions were predominantly metastatic being 39 cases (30.5%), followed by multiple myeloma 12 cases (9.4%), Ewing's sarcoma 8 cases (6.3%), and non-Hodgkins lymphoma 4 cases (3.1%). No cell yield was obtained in 4 cases (3.1%).
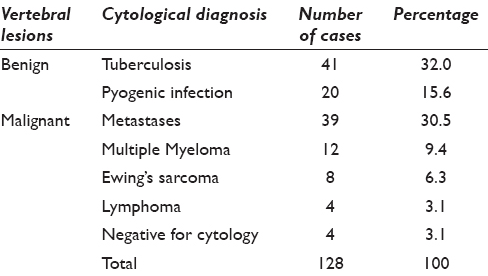
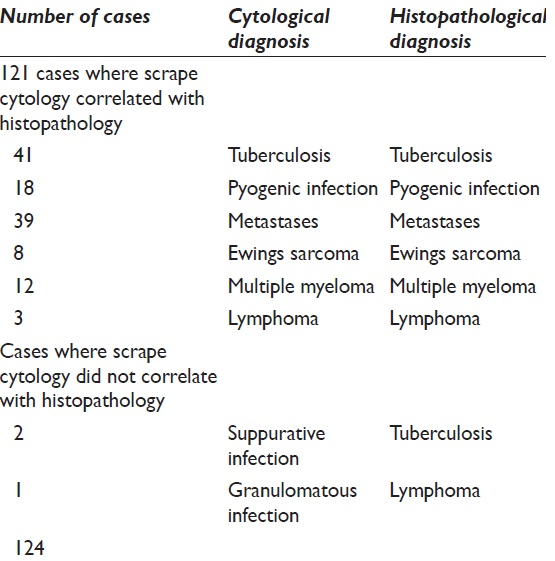
Three cases did not correlate with histopathology [Table 2]. In one case, cell yield in scrape cytology was scanty with fibrous connective tissue elements and macrophages and was reported as granulomatous whereas histology showed a lymphoma with desmoplasia. The other two cases were diagnosed as pyogenic infection due to the large number of neutrophils and macrophages and on histology were found to be granulomatous infection with cold abscess formation. Our study revealed a sensitivity of 97.58%, specificity of 100%, positive predictive value of 100%, and negative predictive value of 33.33%.
DISCUSSION
Scrape smear cytology is a modification of imprint cytology in which cells are harvested by scraping the cut surface of the specimen. It is an economical, simple and quick method of intra-operative diagnosis, and does not alter the utility of the specimen for subsequent histopathology examination.[1]
This technique has been used for various organs including ovary and has been described as an effective, economical, simple, fast and reliable method with results comparable with frozen section diagnosis.[1]
Shidham et al.[6] and Khunamornpong and Siriaunkgul[7] observed that scraping of tumor is the method preferred because a large number of cells can be obtained and cells can be spread well on the slides. Imprint preparation yields less cellular smears than scrape smears. We also found that smears prepared after scraping of material yielded cellular smears and aided in accurate diagnosis.
Representative, adequate material has been a problem in transpedicular vertebral body biopsies resulting in inconclusive diagnosis and delayed management. Intraoperative scrape cytology can be used to confirm the adequacy of the material in addition to the diagnosis hence minimizing the number of negative biopsies.[4] In cases where adequacy was lacking a repeat core biopsy was asked for while the patient was still in the operative room, thus aiding in avoiding a second sitting after a negative histopathological examination. Naresh-Babu et al.[8] have quoted adequacy of biopsy specimens with intraoperative cytology to have a sensitivity of 96.9%, specificity of 100%, positive predictive value of 100%, and negative predictive value of 87.5% in their study. Our study revealed comparable results with studies with a sensitivity of 97.58%, specificity of 100%, positive predictive value of 100% and negative predictive value of 33.33%.
In two similar studies by Kolte and Satarkar, on intraoperative diagnosis of surgically removed specimens, diagnostic accuracy rate was 97.3%[9] and by Sadhana et al. was 93.49%.[10] The usefulness of scrape cytology was demonstrated in lymph nodes in gynecological practice[11] and on sentinel lymph nodes in surgical practice by various studies.[1213]
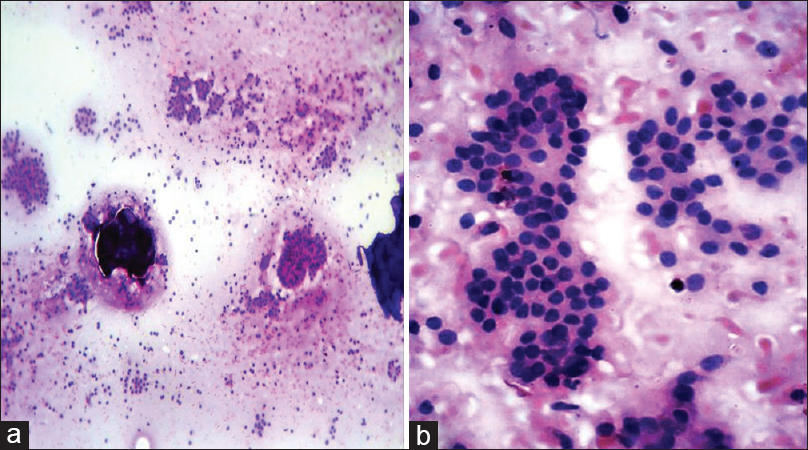
The yield in scrape smears in majority of cases was rich except in cases of lymphoma. The smears of tuberculous infection showed sheets of epithelioid cells along with fibrous connective tissue elements and foreign body type of giant cells [Figure 2a and b].
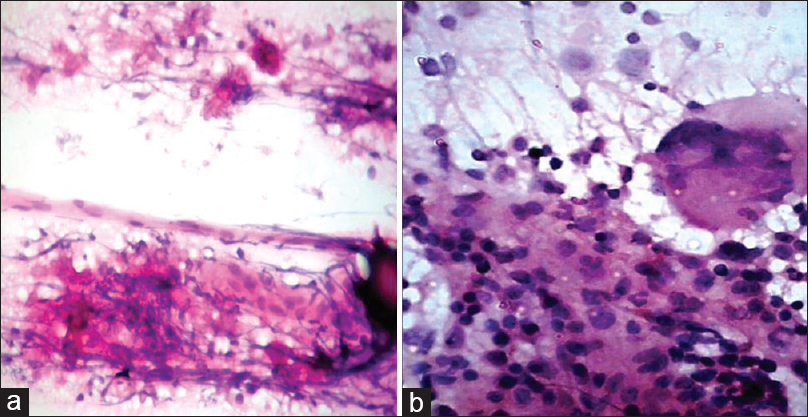
- (a) Scrape smear showing sheets of epithelioid cells along with fibrous connective tissue elements (H and E, ×100). (b) Scrape smear in tuberculous infection with epithelioid cells and foreign body giant cell (H and E, ×400)
Scrape smears from metastatic adenocarcinomatous lesions showed adenocarcinomatous cells in gland patterns with pleomorphic nuclei and high mitotic activity [Figure 3a].
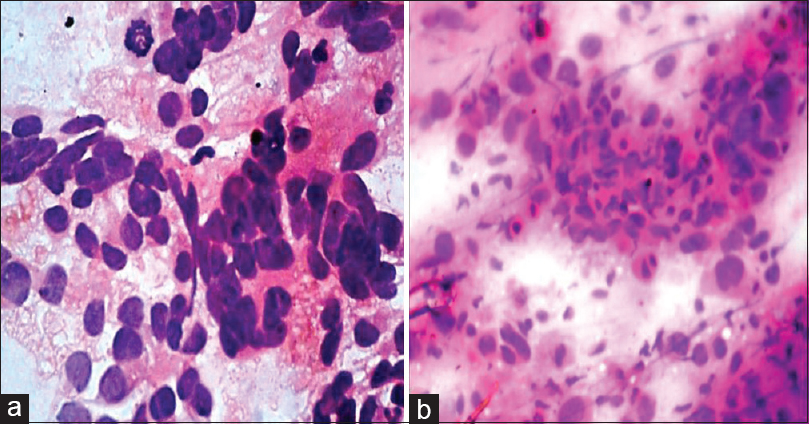
- (a) Scrape smear showing adenocarcinomatous cells in gland patterns with pleomorphic nuclei and also with high mitotic activity (H and E, ×400). (b) Scrape smear of a squamous cell carcinoma metastases with malignant epithelial cells having moderate amount of bright eosinophilic cytoplasm and pyknotic nuclei (H and E, ×400)
Whereas smears from a squamous cell carcinoma metastases were cellular with malignant epithelial cells having moderate amount of bright eosinophilic cytoplasm and pyknotic nuclei [Figure 3b]. A metastatic lesion from a follicular carcinoma of thyroid showed cellular smears with small cells in repetitive and microfollicular patterns, and diagnosis was comparatively easy [Figure 4a and b].
- (a) Scrape smear of metastases from a follicular carcinoma of thyroid showing small cells in follicular patterns (H and E, ×100). (b) Scrape smear higher magnification of the metastases from a follicular carcinoma of thyroid (H and E, ×400)
Scrape smear of a metastatic lesion from an anaplastic carcinoma of thyroid revealed highly pleomorphic cells along with tumor giant cells [Figure 5] whereas cells of a non-Hodgkins lymphoma were monomorphic with smear artifacts [Figure 6a].

- (a) Scrape smear of a metastatic lesion from an anaplastic carcinoma of thyroid (H and E, ×100). (b) Scrape smear of anaplastic carcinoma metastases with highly pleomorphic cells and tumor giant cells (H and E, ×400)
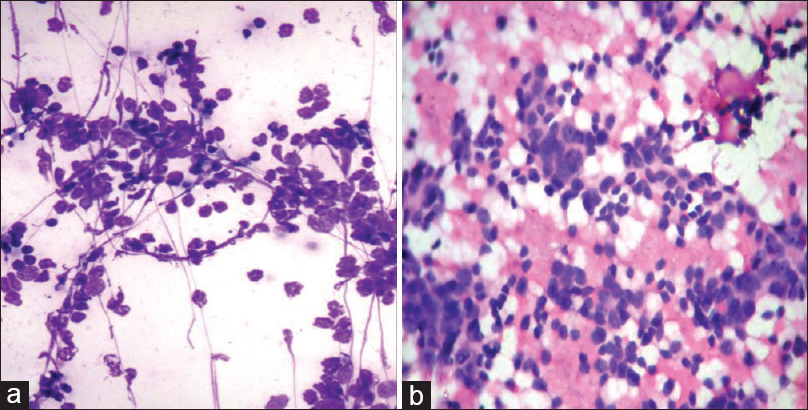
- (a) Scrape smear of a non-Hodgkins Lymphoma with round to oval cells having minimum cytoplasm and smear artifact (H and E, ×400). (b) Scrape smear of Ewing's sarcoma with round cells in vague rosette patterns against a hemorrhagic background (H and E, ×400)
Cells of Ewing's sarcoma were blue and round found in vague rosette patterns against a hemorrhagic background [Figure 6b].
Scrape smears of myeloma were highly cellular and composed of plasma cells, plasmablasts and Mott cells [Figure 7a and b].
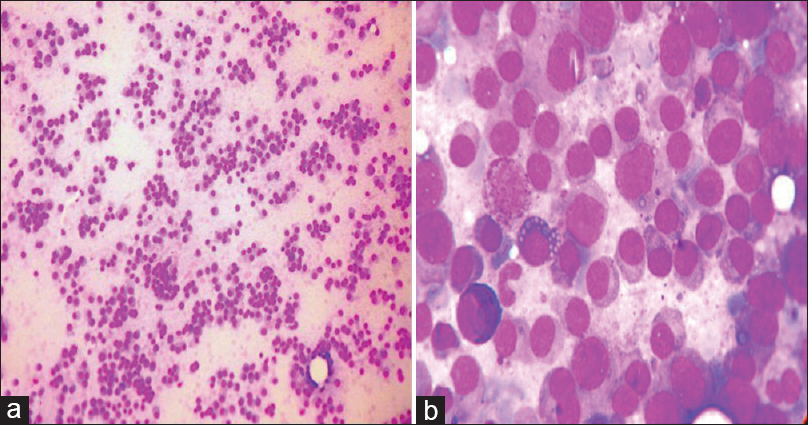
- (a) Scrape smear of myeloma showing high cellularity and composed of cells with eccentric nuclei and moderate amount of cytoplasm (H and E, ×100). (b) Scrape smear of myeloma with plasma cells, plasmablasts and Mott cells (H and E, ×400)
Three of our 124 cases did not correlate with histopathology [Table 2]. With one case showing inadequate cell yield and reported as granulomatous and which on histology turned out to be a lymphoma with desmoplasia. The inadequacy of cell yield was probably the reason for the erroneous diagnosis. The other 2 cases of lymphoma diagnosed also showed scanty cell yield but adequate for an accurate diagnosis. Hence, scanty cell yield should always be viewed cautiously and a repeat core biopsy can be asked for while the patient is still on the table. The other two cases which were reported as pyogenic infection, on histology were found to be granulomatous with cold abscess formation. The large number of neutrophils and macrophages and few epitheloid cells were the cause for the missed diagnosis. The distinction between specific and nonspecific infection is only academic since vertebroplasty is contraindicated in any suspected infection.
The present study evaluates the role of intraoperative cytology in rapid intraoperative diagnosis and hence helps in not only increasing the diagnostic yield of vertebral biopsies but also in aiding to injecting the bone cement in a single sitting. Based on the findings of cytological examination, malignant lesions were subjected to vertebroplasty [Figure 8]. In lesions with infective etiology, vertebroplasty was abandoned, and antibiotic or antituberculous therapy was started. Due to the high cell yield diagnostic accuracy was very good and correlated with the histological diagnosis in majority of cases.
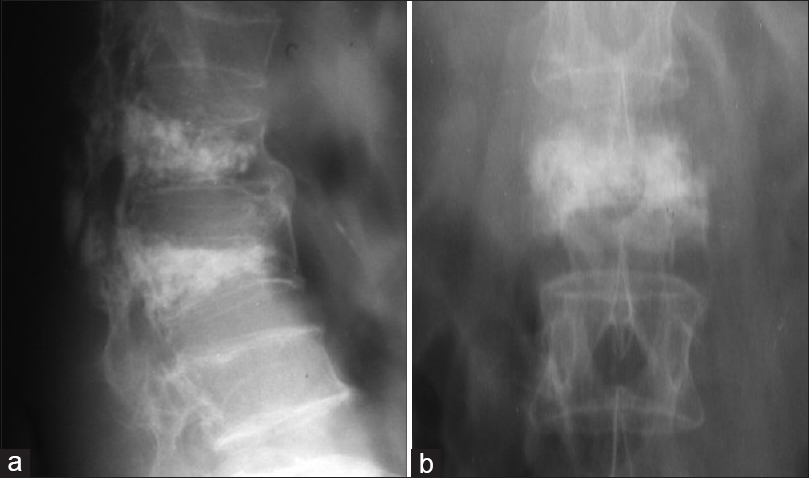
- (a and b) Postoperative images after vertebroplasty was done in a case of vertebral metastases
CONCLUSION
Intraoperative scrape cytology, after transpedicular core biopsy, is a rapid and accurate cytodiagnostic tool, which can be routinely used during vertebroplasty, and injection of bone cement into the pathological vertebral body can be done in the same sitting. To our knowledge, this study is the first in literature to assess the role of this method in rapid diagnosis, and also to aid in assessing adequacy of material for histopathological examination.
COMPETING INTERESTS STATEMENT BY ALL AUTHORS
The author(s) declare that they have no competing interests.
AUTHORSHIP STATEMENT BY ALL AUTHORS
Authorship statement has been signed by all authors
ETHICS STATEMENT BY ALL AUTHORS
Ethical clearance has been issued by the institutional ethical committeee.
LIST OF ABBREVIATIONS (In alphabetic order)
H and E - Hematoxylin and Eosin
MRI - Magnetic Resonance Imaging.
EDITORIAL/PEER-REVIEW STATEMENT
To ensure the integrity and highest quality of CytoJournal publications, the review process of this manuscript was conducted under a double-blind model (authors are blinded for reviewers and vice versa) through automatic online system.
REFERENCES
- Intraoperative scrape cytology: Adult granulosa cell tumor of ovary. J Cytol. 2011;28:207-9.
- [Google Scholar]
- Percutaneous vertebroplasty guided by a combination of CT and fluoroscopy. AJNR Am J Neuroradiol. 1994;15:83-6.
- [Google Scholar]
- Percutaneous vertebroplasty and kyphoplasty for painful vertebral body fractures in cancer patients. J Neurosurg. 2003;98(1 Suppl):21-30.
- [Google Scholar]
- Percutaneous vertebroplasty: A new serial injection technique to minimize cement leak. Asian Spine J. 2015;9:855-62.
- [Google Scholar]
- Percutaneous vertebroplasty: Indications, contraindications, and technique. Br J Radiol. 2003;76:69-75.
- [Google Scholar]
- Role of scrape cytology in rapid intraoperative diagnosis. Value and limitations. Acta Cytol. 1984;28:477-82.
- [Google Scholar]
- Scrape cytology of the ovaries: Potential role in intraoperative consultation of ovarian lesions. Diagn Cytopathol. 2003;28:250-7.
- [Google Scholar]
- Increasing the specimen adequacy of transpedicular vertebral body biopsies. Role of intraoperative scrape cytology. Spine J. 2014;14:2320-5.
- [Google Scholar]
- Role of scrape cytology in the intraoperative diagnosis of tumor. J Cytol. 2010;27:86-90.
- [Google Scholar]
- Scrape cytology in rapid intraoperative diagnosis of tumors. IOSR J Dent Med Sci. 2015;14:65-72.
- [Google Scholar]
- Scrape cytology for intraoperative evaluation of lymph nodes in gynecologic cancer. Obstet Gynecol. 2000;95:67-71.
- [Google Scholar]
- Intraoperative scrape cytology of the sentinel lymph node in patients with breast cancer. Br J Surg. 2002;89:1290-3.
- [Google Scholar]
- Intraoperative examination of sentinel lymph nodes using scrape cytology. S Afr J Surg. 2014;52:75-8.
- [Google Scholar]




