


Translate this page into:
Thyroid fine-needle aspiration of an immunocompromised patient: Cytomorphological clues
*Corresponding author
-
Received: ,
Accepted: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A 25-year-old female with autoimmune hepatitis, primary sclerosing cholangitis, and ulcerative colitis presented to our clinic. She underwent a deceased donor liver transplant in 2014. The patient had a history of multiple thyroid nodules and was evaluated by our endocrinologists. Her thyroid-stimulating hormone (TSH) was normal. An ultrasound of the thyroid was performed and it showed an indeterminate right thyroid nodule of 1.8 cm, along with a couple of small nodules ranging from 0.3 to 0.5 cm. This indeterminate thyroid nodule demonstrated a heterogeneous appearance with multiple hyperechoic foci and subtle posterior shadowing. The multiple hyperechoic foci raised a suspicion for microcalcifications or inspissated colloid on ultrasound. Therefore, a recommendation for ultrasound-guided fine-needle aspiration (FNA) was made.
FNA of the thyroid nodule with Papanicolaou (Pap)-stained preparation showed low-power smears (×10) with some colloid, bland follicular cells, and few multinucleated giant cells [Figure 1].
- Fine-needle aspiration of the thyroid nodule with Papanicolaou-stained preparation
WHAT IS YOUR INTERPRETATION?
-
Benign thyroid nodule with subacute thyroiditis
-
Benign thyroid nodule with Blastomyces infection
-
Benign thyroid nodule with Coccidioides infection
-
Benign thyroid nodule with Aspergillus infection.
ANSWER
The correct cytopathological interpretation is c:
c. Benign thyroid nodule with Coccidioides infection.
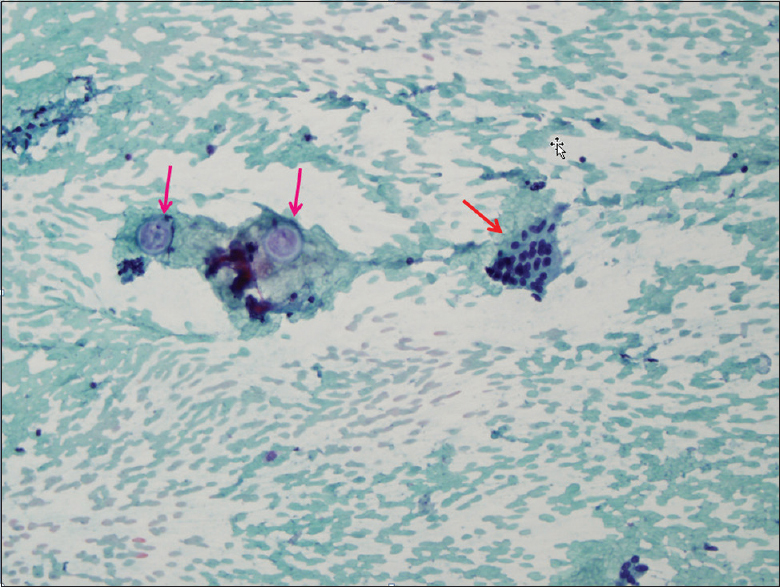
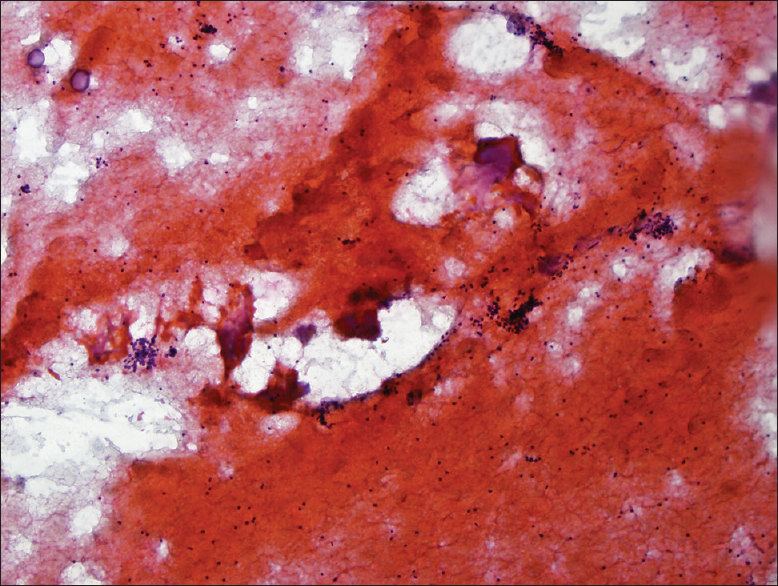
The thyroid FNA shows a background of colloid, bland follicular cells, and a few multinucleated giant cells [Figure 2]. In addition, there are numerous large spherules, ranging from immature, mature to ruptured spherules [Figure 3]. Some of the mature large spherules had the “pink ball” appearance on Pap-stained smears containing endospores [Figure 4]. These findings are quite classic for Coccidioides thyroiditis.
- The thyroid fine-needle aspiration shows a background of colloid, bland follicular cells, and a few multinucleated giant cells

- Numerous large spherules, ranging from immature, mature, to ruptured spherules
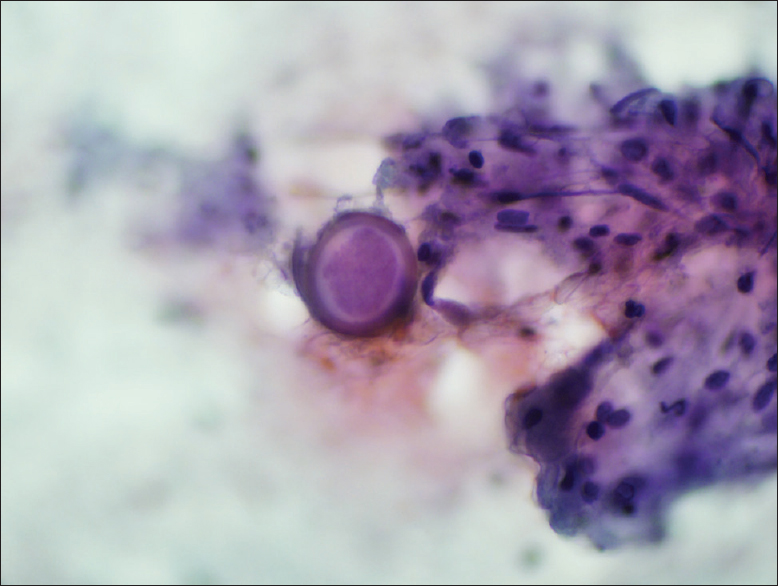
- Some of the mature large spherules having the “pink ball” appearance on Pap-stained smears containing endospores
The other options are explained as follows:
-
The hallmark of subacute (De Quervain's) thyroiditis is the presence of granulomas and multinucleated giant cells engulfing colloid
-
Blastomyces infection is more common in the Southeastern United States, as well as in the Ohio and Mississippi river valley. Blastomyces organisms are 8–15 µm in diameter and have thick, refractile cell walls with a characteristic broad-based budding
-
Aspergillus is characterized by uniform cell walls and true septation fungal hyphae with 45° angle branching.
Features favoring Coccidioides thyroiditis:
-
The patient is immunocompromised and she is from Arizona
-
Numerous nonbudding spherules
-
Thick-walled spherules measuring 20–60 µm
-
Spherules containing endospores
-
Several ruptured and empty spherules.
RADIOLOGICAL CORRELATION AND FOLLOW-UP OF THE PRESENT CASE
Longitudinal [Figure 5a], transverse [Figure 5b], and color Doppler [Figure 5c] images of the right thyroid demonstrate a heterogeneous nodule with ill-defined hyperechoic foci and subtle posterior shadowing (arrows).

- (a-c) Longitudinal (a), transverse (b), and color Doppler (c) images of the right thyroid demonstrate a heterogeneous nodule with ill-defined hyperechoic foci and subtle posterior shadowing (arrows)
The patient subsequently developed military nodules throughout her lung and widespread skeletal involvement by bone scan, consistent with the disseminated coccidioidomycosis. Her serology test was also positive for Coccidioides.
ADDITIONAL QUIZ QUESTIONS
Q1. How the diagnosis of thyroid coccidioidomycosis is made?
-
Histopathology with immunohistochemistry
-
Molecular microbiology
-
A combination of serology, microbiologic culture, and FNA cytology
-
Serum TSH.
Q2. Which of the following cytomorphological feature is highly specific for Coccidioides organisms identified on FNA specimens?
-
Single teardrop-shaped budding fungus highlighted by mucicarmine stain
-
Nonbudding thick-walled spherules containing endospores
-
Broad-based budding yeast with a “snowman” appearance
-
Small nonbudding yeast and it is difficult to recognize with Pap stain.
Q3. Which of the following cytomorphological feature present in this case is not common for Coccidioides?
-
Clean background
-
Multinucleated giant cells
-
Colloid
-
Bland follicular cells.
ANSWERS TO THE ADDITIONAL QUIZ QUESTIONS
A1. c; A2. b; A3. a.
A1. (c) Diagnostic methods for Coccidioides infection typically include serology for antibodies, microbiological culture, and histopathology with special stains.[123] FNA has proven to be a rapid and effective diagnostic procedure of infectious lesions. Some studies emphasize that FNA is an effective diagnostic tool, and clinicians need to be aware of the unique advantages of FNA in the diagnosis of coccidioidomycosis.
The other options are explained as follows:
-
Special stain, such as methenamine silver stain, can highlight Coccidioides. Immunohistochemistry has no value.
-
Microbiologic culture is the routine method.
-
Serum TSH is not the method to diagnose Coccidioides.
A2. (b) One of the classic morphologies of Coccidioides on FNA cytology is nonbudding thick-walled spherule containing endospores.
The other options are explained as follows:
-
Single teardrop-shaped budding fungus highlighted by mucicarmine stain refers to Cryptococcus.
-
Broad-based budding yeast with a “snowman” appearance refers to Blastomyces.
-
Small nonbudding yeast and it is difficult to recognize with Pap stain, this refers to histoplasma capsulatum.
A3. (a) FNA of Coccidioides infection usually shows a “dirty” inflammatory background with acute, chronic, and granulomatous inflammation. It is unusual in this case that the background is relatively clean.
The other options are explained as follows:
(b), (c), and (d) Multinucleated giant cells, colloid, and bland follicular cells are nonspecific findings and usually present in thyroid Coccidioides infection.
BRIEF REVIEW OF THE TOPIC
Coccidioidomycosis is endemic in the arid regions of the United States, such as Arizona and parts of California.[456] Most Coccidioides infections are caused by the inhalation of spores, and its major presentation is that of pulmonary infection.[7] Disseminated pulmonary Coccidioides infection is also quite common, especially among immunocompromised patients.[8] Coccidioidomycosis can rarely manifest as extrapulmonary disease.[9] The most common extrapulmonary sites of involvement are skin, bone, soft tissue, and the central nervous system.[9] However, coccidioidal infection of the thyroid gland is extremely rare with only <10 cases reported in the English literature.
The diagnosis of coccidioidomycosis is often made through a combination of histopathology, microbiology culture, and serology.[10] FNA cytology has proven to be an effective diagnostic tool for infectious lesions. The utility of FNA to diagnose pulmonary coccidioidomycosis has also been well established.[11] Although several case reports have shown coccidioidomycosis of the thyroid gland,[121314] the diagnosis is often made by microbiologic culture, serology, or histology with special stains, this case illustrates that coccidioidomycosis of the thyroid gland can be diagnosed correctly by FNA cytology.
One interesting feature of this case is the presence of multinucleated giant cells. The differential diagnosis of giant cells in a thyroid aspirate includes Hashimoto's thyroiditis, subacute thyroiditis (De Quervain's thyroiditis), papillary thyroid carcinoma (PTC), and infections (tuberculosis, fungus, syphilis, parasites, etc.).[1] Hashimoto's thyroiditis is characterized by Hürthle cells and a background of lymphoid cells, which are not present in our case. The hallmark of subacute thyroiditis is the presence of multinucleated giant cells surrounding and engulfing colloid. Follicular cells tend to be sparse and the background often shows cellular debris and a variable amount of acute and chronic inflammation. Organisms are absent. FNA of PTC can have numerous giant cells. However, in addition to the giant cells, the neoplastic follicular cells show typical features of PTC.
Immunocompromised patients may have multiple infections discovered at the same time.[2] The serology and microbiological culture of the lung lesions of our patient confirm the presence of Coccidioides. No additional fungal organisms or tuberculosis are detected. The rare cases of Blastomyces and Cryptococcus of the thyroid gland have been reported.[23] Blastomyces are broad-based budding organisms (like “snowman”) and have thick cell walls. Cryptococcus is characterized by a single teardrop-shaped budding with a thick mucoid capsule, which can be highlighted by mucicarmine stain. Our case shows the classic morphologic features of Coccidioides.
SUMMARY
-
Although extremely rare, thyroid involvement by Coccidioides can occur
-
FNA of the thyroid is an effective diagnostic tool to establish the diagnosis
-
Pathologists should be aware of the morphologic appearance of coccidioidomycosis on thyroid FNA and search for Coccidioides spherules even in the absence of necrotic debris and inflammation.
COMPETING INTEREST STATEMENT BY ALL AUTHORS
The authors declare that they have no competing interests.
AUTHORSHIP STATEMENT BY ALL AUTHORS
All authors of this article declare that we qualify for authorship as defined by the International Committee of Medical Journal Editors (http://www.icmje.org/#author).
Each author has participated sufficiently in the work and has taken public responsibility for appropriate portions of the content of this article.
ETHICS STATEMENT BY ALL AUTHORS
As this is a quiz case without identifiers, our institution does not require approval from the Institutional Review Board.
LIST OF ABBREVIATIONS (In alphabetic order)
FNA: Fine-needle aspiration
PTC: Papillary thyroid carcinoma
TSH: Thyroid-stimulating hormone.
EDITORIAL/PEER-REVIEW STATEMENT
To ensure the integrity and highest quality of CytoJournal publications, the review process of this manuscript was conducted under a double-blind model (authors are blinded for reviewers and vice versa) through automatic online system.
REFERENCES
- Subacute granulomatous (De Quervain's) thyroiditis: Fine-needle aspiration cytology and ultrasonographic characteristics of 21 cases. Cytojournal. 2015;12:9.
- [Google Scholar]
- Concomitant tuberculous and cryptococcal thyroid abscess in a human immunodeficiency virus-infected patient. Scand J Infect Dis. 2003;35:68-70.
- [Google Scholar]
- Disseminated blastomycosis diagnosed by fine-needle aspiration of the thyroid. Diagn Cytopathol. 2011;39:446-50.
- [Google Scholar]
- Coccidioidomycosis among visitors to a Coccidioides immitis-endemic area: An outbreak in a military reserve unit. J Infect Dis. 1995;171:1672-5.
- [Google Scholar]
- An epidemic of coccidioidomycosis in Arizona associated with climatic changes, 1998-2001. J Infect Dis. 2005;191:1981-7.
- [Google Scholar]
- Risk factors for severe pulmonary and disseminated coccidioidomycosis: Kern County, California, 1995-1996. Clin Infect Dis. 2001;32:708-15.
- [Google Scholar]
- Pulmonary and extrapulmonary coccidioidomycosis, active component, U.S. Armed Forces, 1999-2011. MSMR. 2012;19:2-4.
- [Google Scholar]
- Laboratory aspects in the diagnosis of coccidioidomycosis. Ann N Y Acad Sci. 2007;1111:301-14.
- [Google Scholar]
- Coccidioides thyroiditis in an HIV-infected patient. J Clin Microbiol. 2012;50:2535-7.
- [Google Scholar]




