


Translate this page into:
Overlap syndrome of Erdheim-Chester disease and Langerhans cell histiocytosis: A case report


*Corresponding authors: Guinian Huang, Department of Hematology, Zhongshan City People’s Hospital, Zhongshan, China hgn1997@163.com
Xiaojuan Guo, Department of Hematology, Zhongshan City People’s Hospital, Zhongshan, China guoxiaojuan128@163.com
-
Received: ,
Accepted: ,
How to cite this article: Ding Y, Chen S, Huang G, Guo X. Overlap syndrome of Erdheim-Chester disease and Langerhans cell histiocytosis: A case report. CytoJournal. 2024;21:59. doi: 10.25259/Cytojournal_174_2024
Abstract
Langerhans cell histiocytosis (LCH) and Erdheim–Chester disease (ECD) are exceptionally rare disorders characterized by varied clinical presentations, posing several challenges for clinicians. The concomitant occurrence of LCH and ECD is exceedingly rare and has no known etiology. In this report, we present a rare case of mixed histiocytosis (both ECD and LCH) with multisystem involvement. The patient, a 49-year-old female, initially presented with a rash 2 years ago and progressively developed exophthalmos, fatigue, and shortness of breath. She lacked the mutation in codon 600 of exon 15 of B-Raf proto-oncogene (BRAF-V600E) and subsequently underwent treatment with corticosteroids, interferon-alpha, and chemotherapy, all of which proved ineffective. This work highlights the urgent need to improve treatment outcomes for such patients. Therefore, we discuss the latest advancements in understanding treatment strategies for mixed histiocytic syndromes.
Keywords
Langerhans cell histiocytosis
Erdheim–Chester disease
Histiocytosis

INTRODUCTION
Erdheim-Chester disease (ECD), a rare form of non-Langerhans cell histiocytosis (LCH), typically manifests in middle-aged individuals, primarily males, with rare occurrences in children and the elderly. It is characterized by the infiltration of foamy histiocytes into tissues, which are positive for the cluster of differentiation 68 (CD68) and negative for the cluster of differentiation 1a (CD1a). LCH primarily affects children under 10 years but can affect individuals of all ages. In LCH, the respective tissue-infiltrating histiocytes are positive for CD68 and CD1a. LCH and ECD are mainly triggered by mutations in the mitogen-activated protein kinase/extracellular signal-regulated kinase (MAPK/ERK) pathway, mostly linked to BRAF gene mutations.[1,2]
The clinical presentation of LCH and ECD varies according to the affected sites and the impact on specific organ systems. In ECD, the common symptoms include long bone involvement (80–95%), “hairy kidney” (63%), lung involvement (30–50%), coated aorta (40%), and pseudo-tumoral infiltration of the right atrium (36%).[3] In LCH, bone infiltration is the predominant manifestation (60–80%), followed by lung involvement (15–50%), skin lesions (15–40%), and liver or spleen involvement (15%).[4]
The concomitant occurrence of LCH and ECD has been reported in 15% of patients with ECD.[3] To date, there have been no more than 200 reported cases of mixed ECD–LCH, with only half of them discussing the potential treatment strategies. Given its rarity, no standard treatment exists for mixed histiocytosis, and the prognosis is poor. Herein, we describe an exceptional case of a female patient with mixed histiocytosis lacking the BRAF-V600E mutation who failed to respond to interferon-alpha (IFN-a) and chemotherapy, ultimately leading to her death. Furthermore, we explored the latest developments in treatment strategies for mixed histiocytic syndromes.
CASE REPORT
The study was conducted in accordance with the Declaration of Helsinki and obtained approval from the ethics committee of the institution (protocol code 2022-042) and the informed consent of the patient. A 49-year-old woman with a history of hypertension and diabetes initially presented with a rash [Figure 1a] on the chest, abdomen, and face that started 2 years previously and kept worsening in the recent year. The patient sought medical attention at another hospital. Cranial magnetic resonance imaging (MRI) and magnetic resonance angiography revealed a sellar region mass with changes in both eye sockets, upper maxillary sinuses, and facial structures, accompanied with multiple areas of bone destruction in the maxilla and skull. Despite these findings, no further treatment had been conducted. The patient subsequently developed periorbital xanthelasma [Figure 1b], fatigue, shortness of breath, and exophthalmos.
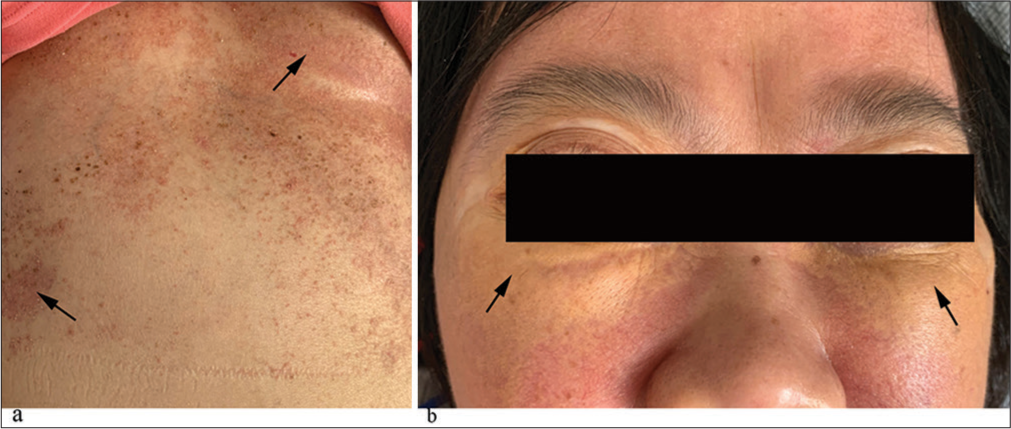
- Characteristic skin manifestations in mixed Erdheim– Chester disease – Langerhans cell histiocytosis. (a) Rash on the skin of the chest and abdomen (black arrows). (b) Bilateral periorbital exophthalmos and xanthelasma-like lesions (black arrows).
In October 2021, the patient was admitted to our institution for further management of multiple serous cavity effusions (pericardial effusion, pleural effusion, and abdominal effusion; [Figure 2a and b]). Orbital computed tomography (CT) indicated soft-tissue masses outside the cone of the extraocular muscles and posterior to the globe in both eye sockets [Figure 2c]. Technetium-99 m bone scintigraphy revealed multiple sites of increased bone metabolism throughout the body (notably bilaterally in the femurs and tibias; [Figure 2d and e]). Contrast-enhanced MRI revealed an abnormal signal of pituitary stalk and bilateral dentate nucleus, local wall thickening and enhancement of the left vertebral artery, and bilateral skin swelling around the eyes [Figure 2f and g].
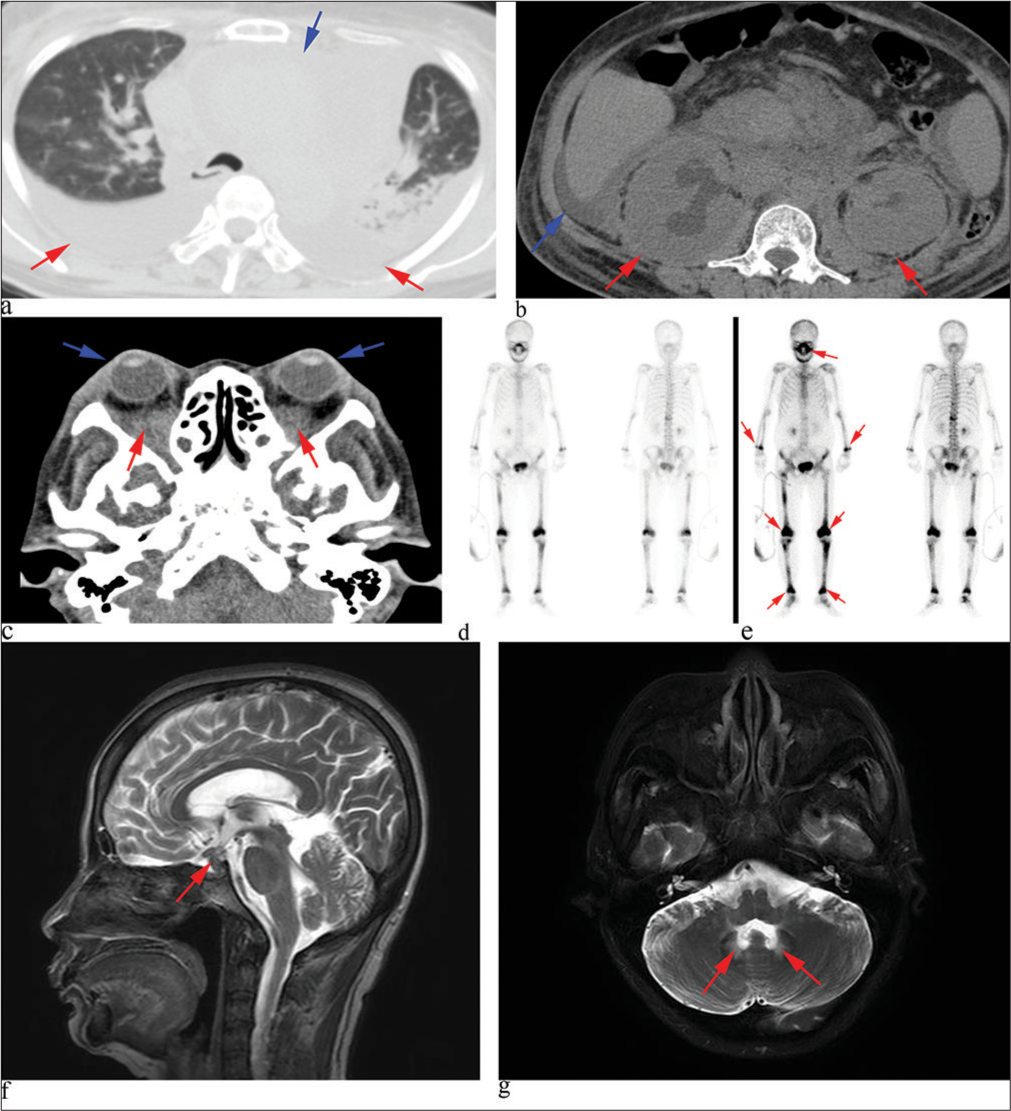
- Clinical imaging before treatments. (a) Chest computed tomography (CT) showed significant pericardial effusion (blue arrow) and bilateral pleural effusion (red arrows). (b) Abdominal CT revealed abdominal effusion (blue arrow) and bilateral kidney enlargement (red arrows). (c) Axial orbital CT indicated bilateral orbital soft-tissue masses (red arrows) and exophthalmos (blue arrows). (d and e) Technetium-99 m bone scintigraphy showed increased bone metabolism at multiple sites, notably in the femurs and tibias bilaterally (red arrows). (f) Sagittal contrast-enhanced magnetic resonance imaging (MRI) T2-weighted imaging (T2WI) revealed an abnormal signal in the pituitary stalk (red arrow). (g) Axial contrast-enhanced MRI T2WI showed high signals in the bilateral dentate nuclei (red arrows).
The patient was diagnosed with ECD, as confirmed by biopsies of the periocular skin and bone marrow, whereas LCH was established from the chest skin. Hematoxylin and eosin staining revealed foamy histiocyte infiltration in the periocular skin [Figure 3a] and bone marrow [Figure 3b], which were consistent with ECD, while a proliferation of Langerhans cells in the chest skin [Figure 3c] was characteristic of LCH. Immunohistochemically, the periocular skin biopsies were positive for CD68 [Figure 4a], but negative for CD1a [Figure 4b] and Langerin [Figure 4c]. Similarly, bone marrow biopsies showed positivity for CD68 [Figure 4d] and were negative for CD1a [Figure 4e]. In addition, the chest skin was negative for acid-fast staining [Figure 4f], excluding mycobacterial infection. By contrast, the LCH lesions were positive for CD68, CD1a, and Langerin [Figure 4g-i]. BRAF V600E mutation was negative in the periocular skin lesion [Figure 5a] and the chest skin lesion [Figure 5b]. The patient’s bone marrow morphology and flow cytometry results excluded a diagnosis of leukemia.
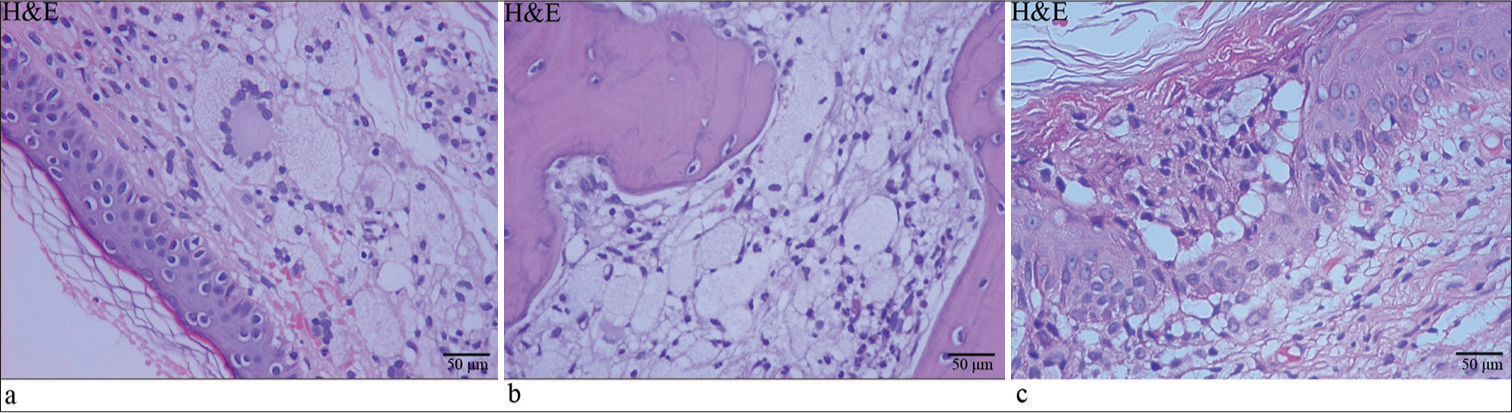
- Hematoxylin and eosin (H&E) staining of mixed Erdheim–Chester disease (ECD)– Langerhans cell histiocytosis (LCH). (a) Periocular skin and (b) bone marrow in ECD with histological changes of multinucleated foamy giant cells. (c) Chest skin in LCH with Langerhans cell aggregates. The magnification of the image was 400×.
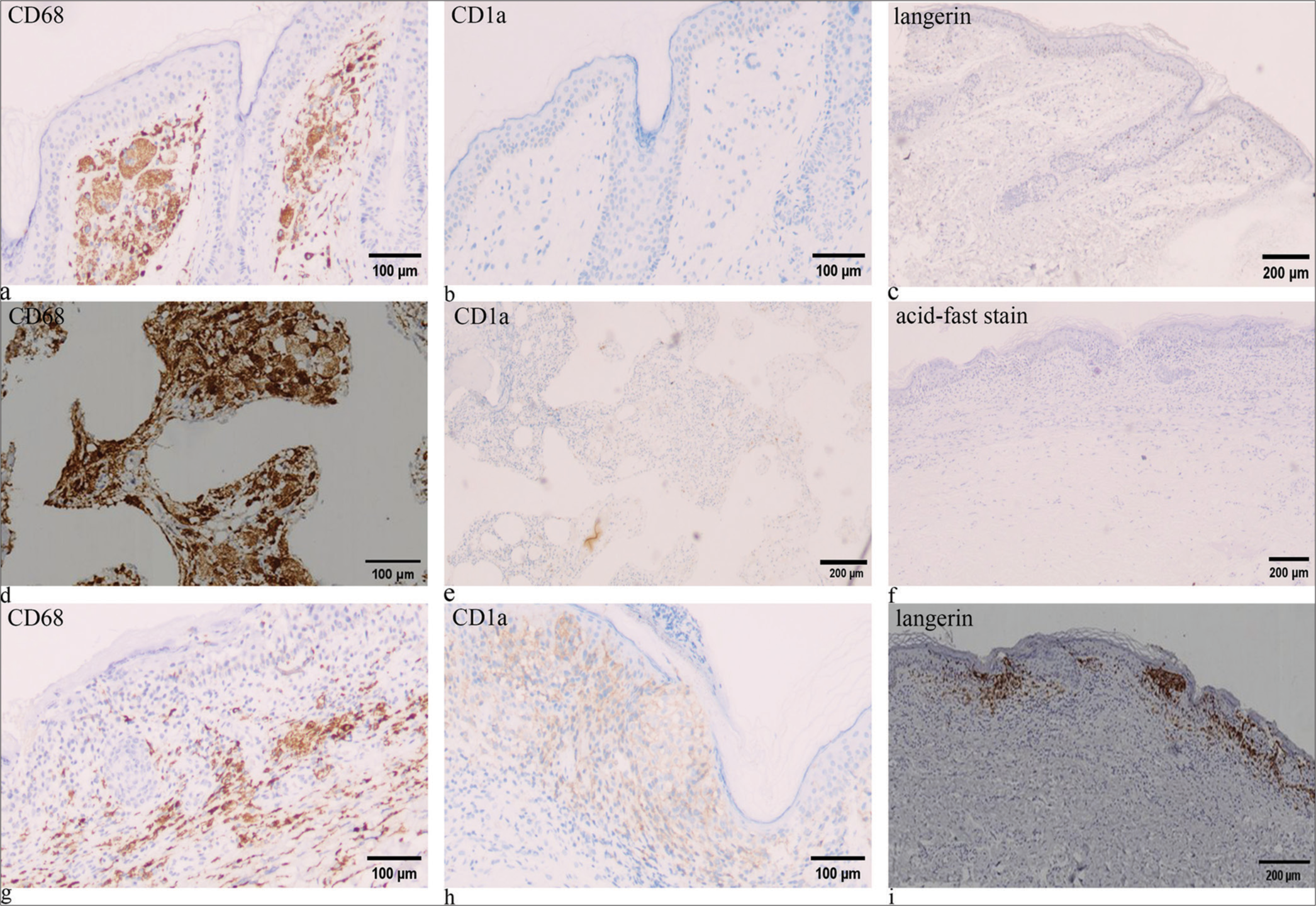
- Immunohistochemical findings in mixed Erdheim–Chester disease–Langerhans cell histiocytosis. (a-c) Cluster of differentiation 68 (CD68) positive, cluster of differentiation 1a (CD1a) negative, and Langerin negative in periocular skin. (d and e) CD68 positive and CD1a negative in bone marrow. (f) Acid-fast stain negative in chest skin. (g-i) CD68 positive, CD1a positive, and Langerin positive in chest skin.
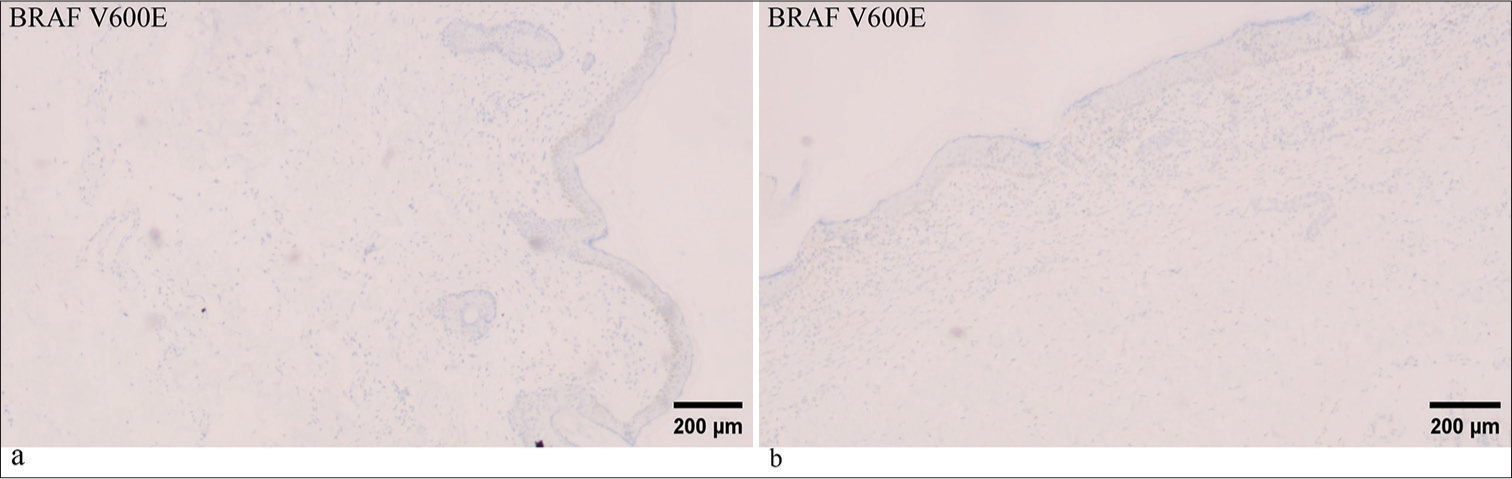
- (a and b) BRAF V600E negative in periocular skin and chest skin respectively. BRAF: B-Raf proto-oncogene, serine/threonine kinase.
The patient was initially subjected to pericardial and pleural effusion drainage, along with treatment with IFN-a to be given as 50 mg subcutaneously every other day and 20 mg of prednisone daily. The symptom of shortness of breath first improved but worsened after 2 months. Follow-up enhanced CT showed multiple soft-tissue masses surrounding the heart, thoracic and abdominal aorta, perirenal space, and mesenteric vascular interspace, along with hydronephrosis in the right renal pelvis and right kidney [Figure 6a and b]. Diffuse bilateral infiltration of the perirenal tissue, known as “hairy kidney,” can cause hydronephrosis and ureteral obstruction. CT of our patient revealed bilateral hairy kidney signs and right hydronephrosis, but renal function remained normal.
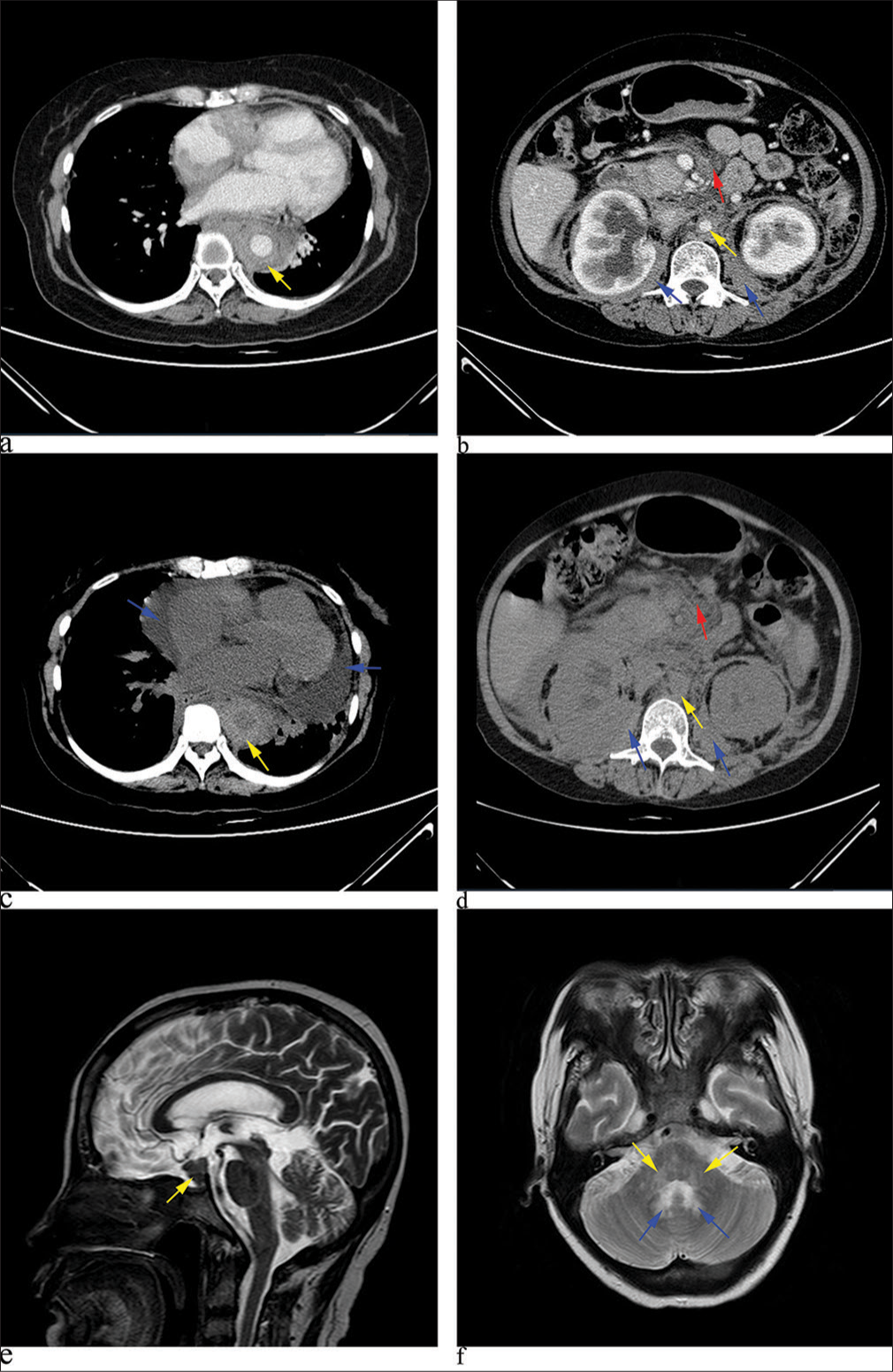
- Clinical imaging during treatments. (a and b) Contrast-enhanced chest and abdominal computed tomography (CT) showed periaortic (yellow arrows), bilateral perinephric (blue arrows), and mesenteric vascular (red arrow) infiltrates. (c) Follow-up CT revealed significant pericardial effusion (blue arrows) and periaortic infiltrates (yellow arrows). (d) The periaortic infiltrates (yellow arrows) were unchanged, while the perinephric (blue arrows) and mesenteric vascular infiltrates (red arrow) increased in density. (e) Follow-up sagittal and axial magnetic resonance imaging T2-weighted imaging demonstrated multiple abnormal signals in the pituitary stalk (yellow arrow), as well as in (f) bilateral dentate nuclei (blue arrows) and pontine arms (yellow arrows), with slight enlargement compared with the previous scan.
As disease progression was assessed, the patient was given the cyclophosphamide, epirubicin, vincristine, prednisone, and etoposide (CHOPE) chemotherapy regimen (1 g of cyclophosphamide on day 1, 100 mg of epirubicin on day 1, 2 mg of vincristine on day 1, 60 mg of prednisone on days 1–5, and 100 mg of etoposide on day 1). The symptoms of chest tightness and shortness of breath improved slightly. After 21 days, another cycle of CHOPE chemotherapy was administered with the same regimen. After treatment, the patient suffered from fever, with the highest temperature of 38.5°C. Blood counts showed grade IV neutropenia (white blood cell: 0.91 × 109/L, neutrophils: 0.28 × 109/L). The level of C reactive protein (CRP) was 136.9 mg/L (0–5 mg/L). Following intervention, the blood counts and body temperature returned to normal, and CRP level decreased to 25.9 mg/L.
Subsequently, the patient underwent a third cycle of CHOPE chemotherapy (same regimen as before). Follow-up CT revealed enlarged soft tissue in the perirenal and mesenteric vascular spaces, along with a significant amount of pericardial effusion [Figure 6c and d]. Reexamination of MRI indicated an enlargement and increase in pituitary lesions compared with previous findings [Figure 6e and f].
Thereafter, the patient experienced recurrent chest tightness, dyspnea, and aggravated lung infection. On March 30, 2022, the patient suffered from sudden cardiac and respiratory arrest. Resuscitation efforts were unsuccessful, and the patient was pronounced dead.
DISCUSSION
A retrospective study reported that over half (51%) of mixed ECD–LCH cases were female, with a median age of symptom onset at 50 years of age. The median follow-up period was 71 months, with a mortality rate of 35%. Mixed histiocytosis tended to involve more multisystem involvement compared with isolated ECD.[5] Our patient was a 49-year-old female. She also exhibited multisystem involvement, affecting the bones, skin, orbits, pituitary, heart, lungs, mesentery, kidneys, and periaortic and perinephric regions. Central nervous system involvement was reportedly linked to poor survival outcomes,[6] as observed in our patient, indicating a poor prognosis.
Mutations in the MAPK pathway, particularly the BRAFV600E mutation, play a key role in the pathogenesis of ECD and LCH. More than 80% patients with mixed histiocytosis carry the BRAF V600E mutation.[6] Therefore, BRAF-V600E mutation testing is recommended for all patients, and targeted-capture next-generation sequencing (NGS) is advised to assess MAPK pathway alterations. Targeted therapies corresponding to these mutations, including BRAF and mitogen-activated extracellular signal-regulated kinase (MEK) inhibitors, have shown promising results in treating LCH and ECD.[7] For patients without the BRAF V600E mutation or those intolerant to BRAF inhibitors, cobimetinib (a MEK inhibitor) has demonstrated an 89% overall response rate in histiocytic disorders.[8] Moreover, a retrospective study showed that BRAF and/or MEK inhibitors are significantly more effective against mixed ECD–LCH, both as first-line (77% vs. 29%, P < 0.001) and across all treatment lines (75% vs. 24%, P < 0.001), compared with conventional treatments (IFN-a, anti-cytokine, and chemotherapy). However, more than half of patients required multiple treatment lines due to disease progression or drug toxicity.[5] In addition, drug resistance and relapse following treatment discontinuation continue to be challenges with current targeted therapies.[9]
For patients without access to targeted therapies, IFN-a is the preferred conventional, evidence-based treatment, with more than half responding positively.[10] However, a significant portion of patients either develop resistance or have to discontinue due to IFN-a intolerance. Before the advent of targeted treatments, systemic chemotherapy is advised for those patients with multisystem LCH. Chemotherapy regimens typically include vinca alkaloid/steroid-based therapies and antimetabolite-based regimens. Although 70– 80% of patients initially respond to vinca alkaloid/steroid-based therapies, 40–80% ultimately experience treatment failure or relapse.[2]
The patient in our case was simultaneously diagnosed with ECD and LCH, lacking the BRAF-V600E mutation, so targeted therapy was not an option. Mixed ECD–LCH exhibited a phenotype more similar to isolated ECD than to isolated LCH,[10] and our patient demonstrated a similar pattern. Therefore, she initially received treatment with IFN-a and prednisolone, but this failed. Chemotherapy treatment was administered subsequently, but this was also ineffective. These findings highlight the challenges in treating mixed histiocytosis, as there is no established standard treatment regimen. In addition, as a result of limitations in our medical facility and the patient’s financial constraints, comprehensive testing for other MAPK pathway mutations, which could have informed further treatment options, was not conducted.
SUMMARY
Conventional treatments proved ineffective for our patient without the BRAF-V600E mutation, leading to a poor prognosis. NGS is recommended to assess other MAPK–ERK pathway alterations that may be amenable to treatment with MEK inhibitors. However, the standard therapeutic approach remains unclear. Diagnosing LCH and ECD sequentially or concurrently may impact treatment decisions. Furthermore, clarification is necessary regarding the selection of first-line therapies; treatment options for refractory or relapsed cases; and the necessity, duration, and dosage of maintenance therapy for post-disease stabilization.
AVAILABILITY OF DATA AND MATERIALS
All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.
ABBREVIATIONS
LCH - Langerhans cell histiocytosis
ECD - Erdheim–Chester disease
BRAF-V600E - The mutation in codon 600 of exon 15 of B-Raf proto-oncogene
IFN-α - Interferon-alpha
CD68 - the cluster of differentiation 68
CD1a - the cluster of differentiation 1a
MAPK/ERK - The mitogen-activated protein kinase/extracellular signal-regulated kinase
MRI - Magnetic resonance imaging
CT - Computed tomography
CHOPE - Cyclophosphamide, epirubicin, vincristine, prednisone, and etoposide
CRP - C reactive protein
NGS - Next-generation sequencing
MEK - Mitogen-activated extracellular signal-regulated kinase
AUTHOR CONTRIBUTIONS
YY D and SS C: Conception and design; XJ G: Administrative support; YY D and XJ G: Provision of study materials or patients; SS C and GN H: Collection and assembly of data; YY D: Data analysis and interpretation; YY D: Data analysis and interpretation; YY D and SS C: Manuscript writing. All authors read and approved the final manuscript.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the Zhongshan City People’s Hospital clinical research and animal experiment (protocol code 2022-042 and date of approval: February 15, 2022). The study obtained the informed consent of the patient.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
EDITORIAL/PEER REVIEW
To ensure the integrity and highest quality of CytoJournal publications, the review process of this manuscript was conducted under a double-blind model (authors are blinded for reviewers and vice versa) through an automatic online system.
FUNDING
Not applicable.
References
- International expert consensus recommendations for the diagnosis and treatment of Langerhans cell histiocytosis in adults. Blood. 2022;139:2601-21.
- [CrossRef] [PubMed] [Google Scholar]
- Histiocytosis and the nervous system: From diagnosis to targeted therapies. Neuro Oncol. 2021;23:1433-46.
- [CrossRef] [PubMed] [Google Scholar]
- Long-term outcome and prognosis of mixed histiocytosis (Erdheim-Chester disease and langerhans cell histiocytosis) EClinicalMedicine. 2024;73:102658.
- [CrossRef] [PubMed] [Google Scholar]
- The clinical spectrum and prognostic factors of Erdheim-Chester disease and mixed Langerhans cell histiocytosis and Erdheim-Chester disease. Ann Hematol. 2023;102:3335-43.
- [CrossRef] [PubMed] [Google Scholar]
- Mixed histiocytic neoplasms: A multicentre series revealing diverse somatic mutations and responses to targeted therapy. Br J Haematol. 2024;205:127-37.
- [CrossRef] [PubMed] [Google Scholar]
- Efficacy of MEK inhibition in patients with histiocytic neoplasms. Nature. 2019;567:521-4.
- [CrossRef] [PubMed] [Google Scholar]
- Targeted therapies in 54 patients with Erdheim-Chester disease, including follow-up after interruption (the LOVE study) Blood. 2017;130:1377-80.
- [CrossRef] [PubMed] [Google Scholar]
- Association of both Langerhans cell histiocytosis and Erdheim-Chester disease linked to the BRAFV600E mutation. Blood. 2014;124:1119-26.
- [CrossRef] [PubMed] [Google Scholar]




