


Translate this page into:
Cytodiagnosis of scar endometriosis
*Corresponding author
-
Received: ,
Accepted: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
Many non-neoplastic and neoplastic lesions that occur on anterior abdominal wall can be confused with scar endometriosis on clinical grounds. Non-neoplastic lesions include hematoma, suture granuloma, abscess, incisional hernia, focal fibrosis, desmoid tumor, keloid and melanocytic nevus. Neoplasms to be differentiated may be primary (benign or malignant) or metastatic (sister Mary Josephs nodule). Scar endometriosis can be differentiated from most of these only on the basis of detailed history about the swelling, careful clinical examination and characteristic cytological features.[1]
We present a case that initially posed a problem in diagnosis as patient could not be seen by the reporting cytopathologist and important clinical indicators were missed. A 35-year-old female patient presented with the complaints of gradually increasing swelling and pain in the infra-umbilical region since last 3 years. Patient did not have swellings at any other site or any other complaints. She gave history of two full term deliveries by cesarean section; her last childbirth was 5 years back.
A 3 cm × 3 cm, firm non-mobile swelling was present on anterior abdominal wall below umbilicus. Skin over the swelling was adherent and discolored [Figure 1]. Clinical diagnosis of soft-tissue tumor was offered and cytology study was advised. Abdominal sonography of patient revealed a poorly defined lesion in the subcutaneous plane with minimal vascularity and without peritoneal communication. The impression given was abdominal wall desmoid.
Fine needle aspiration cytology smears from the tender infraumbilical swelling showed high cellularity of glandular and stromal cells [Figure 2]. Glandular cells were arranged in tight clusters and sheets, had round nuclei with uniform chromatin pattern [Figure 3]. Altered blood, debris and foamy macrophages were seen in the background [Figure 4]. Some macrophages showed presence of hemosiderin pigment.

- Anterior abdominal wall swelling 3×3 cm with discoloured overlying skin near a scar mark
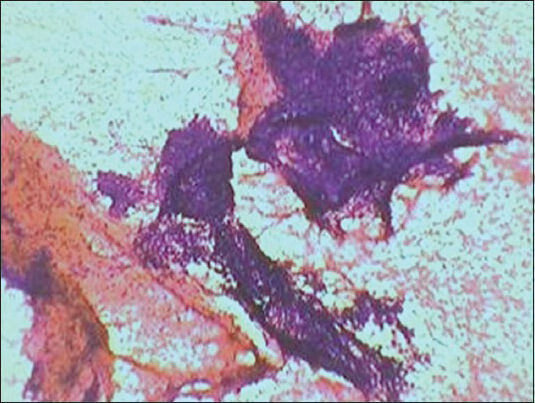
- Bimodal population of endometrial glandular and stromal cells seen as compact fragments in haemorrhagic background (PAP ×100)
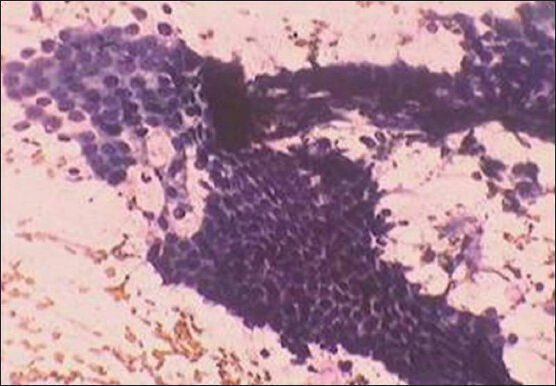
- Honeycomb sheets of glandular cells without nuclear atypia (PAP ×400)
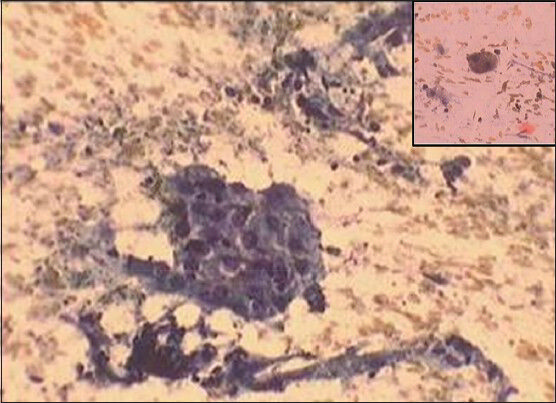
- A group of macrophages in the background of blood and debris (PAP ×400) Inset-Hemosiderin laden macrophage
High cellularity in a dirty background observed in cytology smears initially puzzled us. After carefully examining the swelling and eliciting, the history of increase in the size of the swelling and pain during the menstrual cycle:
-
Noticing the location of the swelling near a scar mark and
-
Appreciating the bland nuclear pattern in glandular and stromal cells in all the smears diagnosis of scar endometriosis could be given.
Endometriosis is defined as the presence of functioning endometrium outside the uterus. Occurrence of endometriosis is described usually in the pelvic region and in many unusual and uncommon extra pelvic sites.[2] Only cutaneous and subcutaneous endometriosis are easily accessible to cytological study. Scar endometriosis-a form of cutaneous endometriosis is generally seen in women of reproductive age group.[3] History of catamenial exacerbation, i.e., increase in pain and tenderness in a lump during menstruation and location of a firm, tender swelling near a scar either of C section, laparotomy, hysterectomy or episiotomy point toward the diagnosis of scar endometriosis.[4] On radiological examination, the swelling is in the subcutaneous plane with no intraperitoneal communication.
Characteristic cytological features include good cellularity of glandular and stromal cells with uniform, bland nuclei in the background of altered blood, debris and foamy macrophages, some of them containing hemosiderin. The cytological features of endometriosis are related to cyclic hormonal changes. In proliferative phase, glandular cells are seen as honeycomb sheets and tight clusters, have round or oval nuclei with evenly distributed chromatin. Stromal cells form syncytial clusters and have plump spindle nuclei with fine chromatin. In the secretory phase, glandular cells show an increase in cell size and microvacuolation while stromal cells reveal abundant cytoplasm.[4]
Diagnosis of endometriosis is not always straight forward. Difficulties arise when it arises in unusual clinical setting and without characteristic bimodal pattern in the smears. When atypical cytological features are seen in smears histological examination is advisable in order to differentiate endometriosis from malignancy.[5]
Fine needle aspiration cytology remains a reliable and relatively atraumatic investigation for primary pre-operative diagnosis in most cases if the cytopathologist is aware of the entity and interprets the cytological features in the light of clinical findings of:
-
A reproductive age group female with discolored swelling near a scar mark on anterior abdominal wall
-
History of catamenial exacerbation
-
Location of swelling in the subcutaneous plane on radiological examination.
Cytology is a method of choice to monitor treatment and possible malignant transformation in a case of endometriosis.
COMPETING INTEREST STATEMENT BY ALL AUTHORS
The author declare that they have no competing interests.
AUTHORSHIP STATEMENT BY ALL AUTHORS
All authors of this article declare that we qualify for authorship as defined by ICMJE http://www.icmje.org/#author.
Each author has participated sufficiently in the work and takes public responsibility for appropriate portions of the content of this article.
Each author acknowledges that this final version was read and approved.
ETHICS STATEMENT BY ALL AUTHORS
This study was conducted with approval from Institutional Review Board (IRB) of the institution associated with this study.
Authors take responsibility to maintain relevant documentation in this respect.
EDITORIAL/PEER-REVIEW STATEMENT
To ensure the integrity and highest quality of CytoJournal publications, the review process of this manuscript was conducted under a double blind model (authors are blinded for reviewers and vice versa) through automatic online system.
REFERENCES
- Uterus-corpus. In: Rosai and Ackerman's Surgical Pathology (10th ed). St. Louis: Mosby; 2012. p. :1486-7.
- [Google Scholar]
- Skin and subcutis. In: Fine Needle Aspiration Cytology (4th ed). New Delhi: Churchill Livingstone; 2005. p. :396.
- [Google Scholar]
- Fine-needle aspiration cytology of scar endometriosis: Study of seven cases and literature review. Diagn Cytopathol. 2011;39:18-21.
- [Google Scholar]
- Primary umbilical endometriosis-Diagnosis by fine needle aspiration. J Cytol. 2011;28:214-6.
- [Google Scholar]




