


Translate this page into:
Impact of the Paris system for reporting urine cytopathology on predictive values of the equivocal diagnostic categories and interobserver agreement
*Corresponding author
-
Received: ,
Accepted: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
The Paris System (TPS) acknowledges the need for more standardized terminology for reporting urine cytopathology results and minimizing the use of equivocal terms. We apply TPS diagnostic terminologies to assess interobserver agreement, compare TPS with the traditional method (TM) of reporting urine cytopathology, and evaluate the rate and positive predictive value (PPV) of each TPS diagnostic category. A survey is conducted at the end of the study.
Materials and Methods:
One hundred urine samples were reviewed independently by six cytopathologists. The diagnosis was rendered according to TPS categories: negative for high-grade urothelial carcinoma (NHGUC), atypical urothelial cells (AUC), low-grade urothelial neoplasm (LGUN), suspicious for high-grade urothelial carcinoma (SHGUC), and high-grade urothelial carcinoma (HGUC). The agreement was assessed using kappa. Disagreements were classified as high and low impacts. Statistical analysis was performed.
Results:
Perfect consensus agreement was 31%, with an overall kappa of 0.362. Kappa by diagnostic category was 0.483, 0.178, 0.258, and 0.520 for NHGUC, AUC, SHGUC, and HGUC, respectively. Both TM and TPS showed 100% specificity and PPV. TPS showed 43% sensitivity (38% by TM) and 70% accuracy (66% by TM). Disagreements with high clinical impact were 27%. Of the 100 cases, 52 were concurrent biopsy-proven HGUC. The detection rate of biopsy-proven HGUC was 43% by TPS (57% by TM). The rate of NHGUC was 54% by TPS versus 26% by TM. AUC rate was 23% by TPS (44% by TM). The PPV of the AUC category by TPS was 61% versus 43% by TM. The survey showed 33% overall satisfaction.
Conclusions:
TPS shows adequate precision for NHGUC and HGUC, with low interobserver agreement for other categories. TPS significantly increased the clinical significance of AUC category. Refinement and widespread application of TPS diagnostic criteria may further improve interobserver agreement and the detection rate of HGUC.
Keywords
Atypical urothelial cells
classification systems for reporting urine cytopathology
interobserver agreement
The Paris System
urine
urine cytology

INTRODUCTION
Urine cytology, much like the gynecologic screening Pap test prior to The Bethesda System in 1988 and thyroid fine-needle aspirations before 2007, suffers from a variable, nonstandardized, and often equivocal terminology. Many classification systems have been proposed since Papanicolaou's proposal in 1947 in an attempt to standardize the diagnostic terminology; however, none have gained widespread implementation. Urine cytology detects high-grade urothelial carcinoma (HGUC) with high specificity and is still the best and most reliable screening test for this condition. The Paris System (TPS) was developed on this principle, essentially to prioritize the detection of high-grade urothelial lesions and standardize the diagnostic terminology based on the underlying histopathology and clinical outcomes, in hopes of minimizing the use of equivocal terms such as “atypical” and “suspicious,” thus facilitating clinical decision-making.[1] For TPS to be widely implemented and for it to endure the test of time, its diagnostic utility and clinical effectiveness should be continuously validated. Since TPS was published in 2016, a number of institutional studies have been published, studying the application of all or some of TPS diagnostic criteria, some with conflicting results.[2345678910] Fewer studies have assessed interobserver agreement.[1112]
In this study, in addition to assessing the interobserver reproducibility (precision), we studied the overall predictive value and detection rate of biopsy-proven high-grade malignancy of TPS in comparison to the traditional method (TM). Predictive value or risk of malignancy by TPS diagnostic category was also studied. The impact of misclassification on clinical management was evaluated. TPS, its sensitivity, specificity, and accuracy for detecting HGUC in comparison to the TM were studied. Finally, a survey was conducted at the end of this study to evaluate the practicality of using TPS by the six participating cytopathologists.
MATERIALS AND METHODS
The study design was reviewed by the Institutional Review Board at Cedars-Sinai Medical Center (CSMC) for compliance with the hospital's national and international standards and designated as “exempt.” An extensive review of the extant literature on urine cytopathology and TPS was conducted. The pathology laboratory database (PowerPath, Sunquest Information Systems, Tucson, AZ, USA) was queried for cytopathology urine samples with concurrent or follow-up surgical biopsies with malignant (HGUC) or benign (non-HGUC) diagnoses performed within a period of up to 3 months. Only cases satisfactory for cytologic evaluation with well-fixed, well-prepared, liquid-based preparations were accepted for inclusion in this study. One hundred urinary cytology samples from 100 patients obtained over 5 years (2013–2017) were selected. All specimens were Papanicolaou stained SurePath® preparations. Each cytology case was independently reviewed by six cytopathologists from the Department of Pathology at CSMC, blinded to the previous cytology and surgical pathology diagnoses and the diagnoses of the other participating cytopathologists. The cytopathologists had between 6 and 25 years' experience with interpreting urine cytopathology at the time of review of study cases. Each cytopathologist rendered a diagnosis according to five TPS categories: negative for HGUC (NHGUC), atypical urothelial cells (AUC), low-grade urothelial neoplasm (LGUN), suspicious for HGUC (SHGUC), and HGUC [Figure 1].[13]
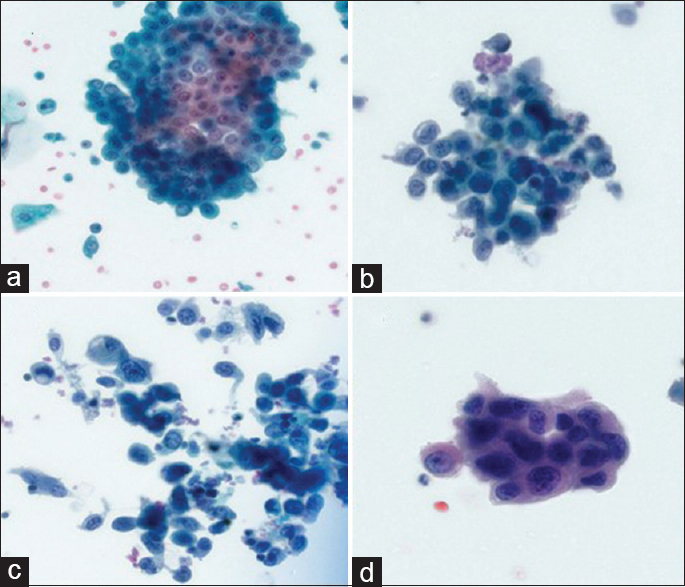
- The Paris System categories. Negative for high-grade urothelial carcinoma (a), atypical urothelial cells (b), suspicious for high-grade urothelial carcinoma (c), and high-grade urothelial carcinoma (d)
The six review cytopathologists had not been involved in the development of TPS; however, each cytopathologist received training on its application (one Grand Rounds presentation by Dr. Guliz Barkan, one College of American Pathologists webinar, two internal PowerPoint presentations, TPS textbook, and a handout summarizing TPS criteria). The nuclear–cytoplasmic (N/C) ratio was estimated visually using the definitions published by TPS. The category LGUN was recognized as a subcategory of NHGUC and was only used where papillary groups of urothelial cells were present with well-defined fibrovascular cores.
The agreement was assessed using kappa. Disagreements were classified as high and low impacts depending on the potential impact of a misclassification on clinical management. High impact was defined as disagreement between categories SHGUC or HGUC versus categories NHGUC, LGUN and AUC, whereas low impact was defined as disagreement among categories NHGUC, LGUN, and AUC. Sensitivity and specificity were assessed by dichotomizing the traditional and TPS diagnostic categories as benign or malignant among majority consensus agreement and comparing them to concurrent surgical biopsies. The decision to include the atypical and low-grade categories in both TM and TPS in the dichotomized benign category was based on what is currently hypothesized about the pathogenetic bases of urothelial carcinoma.[13] The biopsy diagnoses were used as the gold standard and were classified as “biopsy-proven HGUC” and “biopsy-proven non-HGUC,” the latter including biopsy-proven benign and low-grade urothelial carcinoma cases.
A consensus diagnosis for TPS among the six cytopathologists was obtained by the majority consensus diagnosis for each case. The consensus TPS diagnoses were classified as “benign,” a category that included NHGUC, LGUN, and AUC, versus “malignant,” a category that included SHGUC and HGUC.
The TM diagnoses were classified as “malignant,” a category that included HGUC and SHGUC, versus “benign,” a category that included no malignant cells identified, atypical cells present, and low-grade urothelial carcinoma.
At the end of the review, a survey was conducted to assess the ease of implementing the criteria detailed in TPS, its practical benefit, and overall satisfaction.
Statistical analysis
Categorical variables were reported as counts, relative frequencies, and percentages and compared across the two methods by McNemar's test for related proportions. The agreement was assessed by kappa statistics with associated 95% confidence intervals (CI). A two-sided 0.05 significance level was used throughout. Statistical calculations were made using SAS version 9.4 (SAS Institute, Cary, NC, USA).
RESULTS
Of the 100 cases reviewed, 70 were voided and 30 were instrumented (washings/catheterized). They included 26 (26%) negative for malignant cells, 44 (44%) atypical, 11 (11%) suspicious for HGUC, and 19 (19%) HGUC cases diagnosed by TM. Fifty-three percent were concurrent surgical biopsy-proven HGUC and 47 (47%) were biopsy-proven non-HGUC (31 benign and 16 low-grade urothelial carcinoma by surgical biopsy). TPS diagnoses were 54 (54%) NHGUC, 23 (23%) AUC, 9 (9%) SHGUC, and 14 (14%) HGUC. None of the cases were cytologically diagnosed as LGUN or low-grade urothelial carcinoma or other malignancy by either system. There was a perfect agreement among 31% of the cases, with an overall kappa = 0.362 (P < 0.0001, 95% CI: 0.331–0.394). The overall kappa was 0.411 after collapsing the SHGUC and HGUC into one diagnostic category. Among cases with disagreements, 17% (12/69 cases) fell under disagreements with high clinical impact and 65% (45/69 cases) fell under disagreements with low clinical impact. Kappa values by TPS diagnostic category were only significant for the NHGUC category (kappa = 0.483, P < 0.0001, 95% CI: 0.432–0.533) and the HGUC category (kappa = 0.520, P < 0.0001, 95% CI: 0.470–0.571) [Table 1].
| TPS diagnostic category | κ* |
|---|---|
| NHGUC | 0.483 |
| AUC | 0.178 |
| SHGUC | 0.258 |
| HGUC | 0.520 |
| Overall | 0.362 |
| Overall after combining SHGUC and HGUC | 0.411 |
*Kappa values are statistically significant (P<0.0001) for overall kappa, NHGUC and HGUC categories. HGUC: High-grade urothelial carcinoma, NHGUC: Negative for HGUC, AUC: Atypical urothelial cell, SHGUC: Suspicious for HGUC, TPS: The Paris System
Both TM and TPS showed high specificity (100% for both) and high positive predictive value (PPV) (100% for both) for detecting HGUC. TPS showed slightly higher sensitivity at 43% (compared to 38% for TM) and accuracy at 70% (compared to 66% for TM). The detection rate of biopsy-proven HGUC was higher by TM at 57% versus 43% by TPS [Table 2].
| TPS, n (%) | TM, n (%) | |
|---|---|---|
| Sensitivity | 23/53 (43) | 20/53 (38) |
| Specificity | 47/47 (100) | 47/47 (100) |
| PPV | 23/23 (100) | 19/19 (100) |
| NPV | 47/77 (61) | 47/81 (58) |
| Accuracy | 70/100 (70) | 66/100 (66) |
| The detection rate of biopsy-proven HGUC | 23/53 (43) | 30/53 (57) |
HGUC: High-grade urothelial carcinoma, PPV: Positive predictive value, NPV: Negative predictive value, TPS: The Paris System, TM: Traditional method
Out of the 54 cases classified as NHGUC by TPS, 16 (30%) were biopsy-proven HGUC and 38 (70%) were biopsy-proven non-HGUC. The 16 biopsy-proven HGUC cases were classified as 3 negatives, 12 atypical, and 1 suspicious by TM. Of the 23 cases diagnosed as AUC by TPS, 14 (61%) were biopsy-proven HGUC and 9 (39%) were biopsy-proven non-HGUC. All the 9 cases diagnosed as SHGUC and all the 14 cases diagnosed as HGUC (100% each) by TPS were biopsy-proven HGUC [Table 3].
| Diagnostic category | Biopsy-proven HGUC (n=53), n (%) | Biopsy-proven non-HGUC (n=47), n (%) | ||
|---|---|---|---|---|
| TPS | TM | TPS | TM | |
| NHGUC | 16 (30) | 4 (15) | 38 (70) | 22 (85) |
| AUC | 14 (61) | 19 (43) | 9 (39) | 25 (57) |
| SHGUC | 9 (100) | 11 (100) | 0 (0) | 0 (0) |
| HGUC | 14 (100) | 19 (100) | 0 (0) | 0 (0) |
HGUC: High-grade urothelial carcinoma, TPS: The Paris System, TM: Traditional method, NHGUC: Negative for HGUC, AUC: Atypical urothelial cell, SHGUC: Suspicious for HGUC
Fifty-four percent (54/100) of the samples were diagnosed as NHGUC by TPS compared to 26% (26/100) diagnosed as negative for malignant cells by TM (P < 0.0001). In TM, 44% (44/100) of the samples were diagnosed as “atypical cells present” versus 23% (23/100) diagnosed as AUC by TPS (P < 0.0001). No significant difference was noted in the number of cases diagnosed as suspicious by TM (11%, 11/100) versus TPS (9% (9/100) or the number of cases diagnosed as HGUC by TM (19%, 19/100) versus TPS (14%, 14/100), although a decrease in the rate of both categories using TPS is observed [Table 4].
| TPS (n=100) | TM (n=100) | |||
|---|---|---|---|---|
| Negative (n=26) | Atypical (n=44) | Suspicious (n=11) | Malignant (n=19) | |
| NHGUC (n=54) | 25/54 (46) | 28/54 (52) | 1/54 (2) | 0/54 (0) |
| AUC (n=23) | 1/23 (4) | 15/23 (65) | 3/23 (13) | 4/23 (17) |
| SHGUC (n=9) | 0 | 1/9 (11) | 5/9 (56) | 3/9 (33) |
| HGUC (n=14) | 0 | 0 | 2/14 (14) | 12/14 (86) |
HGUC: High-grade urothelial carcinoma, NHGUC: Negative for HGUC, AUC: Atypical urothelial cell, SHGUC: Suspicious for HGUC, TPS: The Paris System, TM: Traditional method
Sixteen (30%) cases diagnosed as NHGUC by TPS were concurrent biopsy-proven HGUC. Three out of those 16 cases were also called negative by TM, 12 were called atypical, and 1 case was called suspicious. All the 16 cases were re-reviewed by the first and last authors (RB and SB). The NHGUC diagnosis was confirmed in 11/16 cases (true negative), whereas five were reclassified as atypical. Eight out of the 11 confirmed negative cases either had clusters of small cells (bland) in voided urine or clusters of basal urothelial cells (washings). The discrepancy in diagnosis of the remaining 3/11 cases (called negative by both TPS and TM) compared to biopsy was attributed to sampling effect. Reclassification of 5/16 cases from NHGUC to atypical after re-review was due to the presence of either rare cell with an only slight increase in N/C ratio or focal subtle atypical features in a background of either inflammation, crystals, or degenerative changes. Figure 2a–d shows the details on subtle atypical findings from each case.
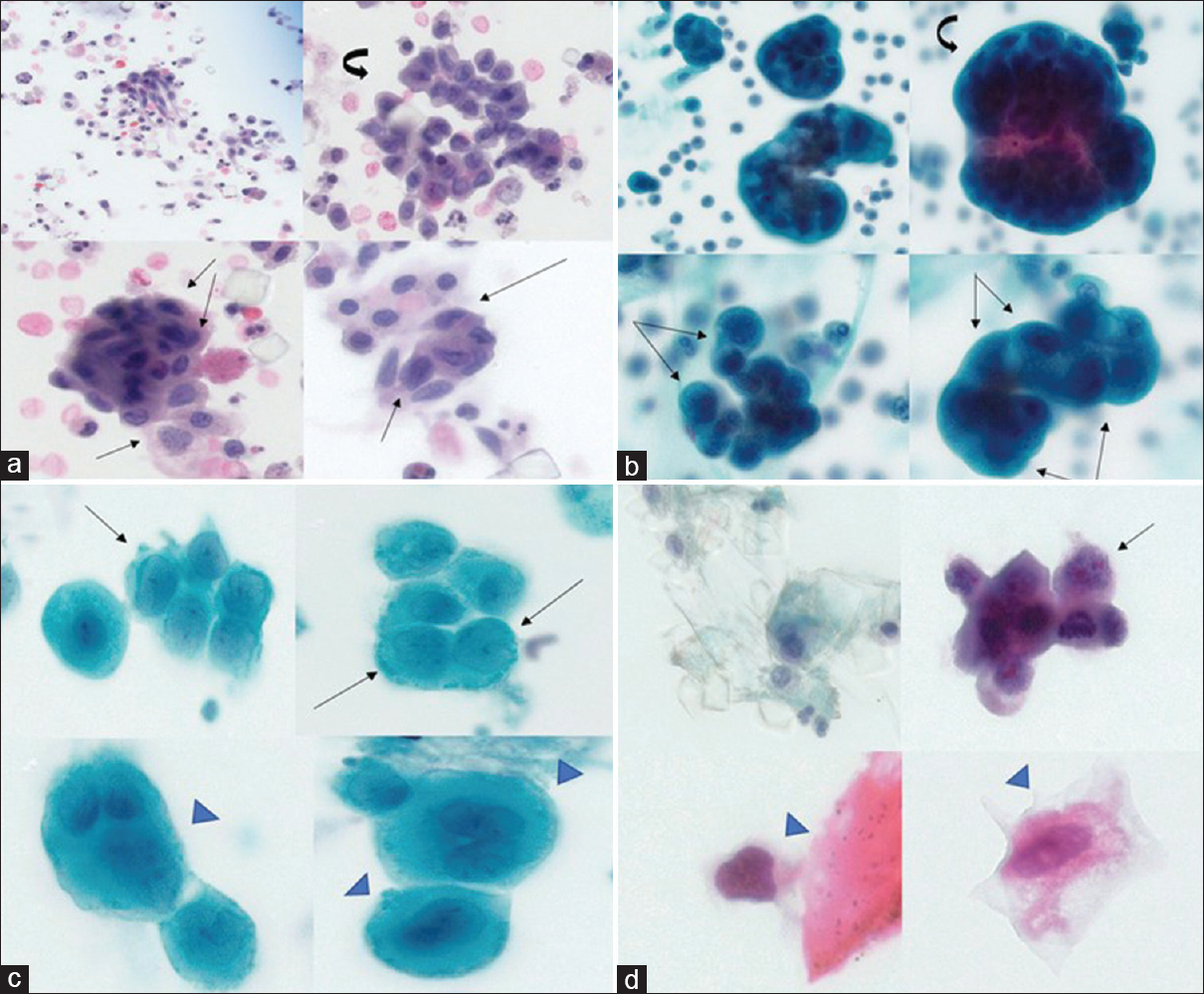
- Focal subtle atypia in biopsy-proven high-grade urothelial carcinoma cases with initial negative high-grade urothelial carcinoma, (a) acute inflammation, crystals, reactive cells (curved arrow). Nuclear–cytoplasmic ratio >0.5, hyperchromasia, membrane irregularity (arrow), (b) acute inflammation, reactive cells (curved arrow). Nuclear–cytoplasmic ratio >0.5, hyperchromasia, nuclear membrane irregularity (arrow), (c) nuclear–cytoplasmic ratio >0.5, nuclear irregularity (arrow). Enlarged nuclei, membrane irregularity, nuclear–cytoplasmic ratio <0.5 (arrowhead), and (d) crystals, acute inflammation, nuclear hyperchromasia, irregularity (arrow). Degenerated cells with irregular nuclei, nuclear–cytoplasmic ratio ≤ 0.5 (arrowhead)
Sixty-seven percent of participating cytopathologists indicated that TPS has influenced their clinical practice or helped improve their diagnostic skills and decreased the rate of AUC diagnosis in the survey taken. The overall satisfaction with TPS was 33%. Challenges that were listed by the cytopathologists included strictly applying the N/C ratio criteria. The majority found that N/C ratio cutoffs of 0.5 versus 0.4 to differentiate between AUC versus NHGUC and N/C cutoffs of 0.5 and 0.6 to differentiate between AUC versus SHGUC were quite challenging. Severe nuclear hyperchromasia and N/C ratio >0.7 as requirements to call SHGUC or HGUC were the limiting factors in some cases that met all other criteria listed in these categories [Figure 3]. Survey results are summarized in Table 5.

- Biopsy-proven high-grade urothelial carcinoma not meeting required criteria by The Paris System of nuclear–cytoplasmic ratio >0.7 (a) and severe nuclear hyperchromasia (b)
| Survey question | Survey result |
|---|---|
| 1. Rate how helpful the diagnostic criteria proposed by TPS for considering the diagnosis of NHGUC? | 67% found criteria for reactive, lithiasis and therapy changes helpful 50% found criteria for benign urothelial tissue fragments and cases that have some cytologic features of LGUN that can be included in the NHGUC category helpful |
| 2. Rate how helpful the diagnostic criteria proposed by TPS for making the diagnosis of AUC? | 17% found N/C ratio criterion helpful 67% found the other criteria helpful |
| 3. Rate how helpful the diagnostic criteria proposed by TPS for considering the diagnosis of LGUN? | 17% found the 3D clusters and the nuclear membrane irregularity criteria helpful |
| 4. Rate how helpful the diagnostic criteria proposed by TPS for making the diagnosis of SHGUC and HGUC? | 50% found N/C ratio and 5-10 cell cutoff criteria helpful 83%-100% found nuclear hyperchromasia, clumped chromatin, and markedly irregular membrane criteria helpful |
| 5. Rate your overall satisfaction with the diagnostic criteria proposed by TPS | 33% overall satisfaction |
| 6. Do you feel the TPS has influenced you to change your urine cytology practice or improve your diagnostic skills (yes or no)? Why? | 67% reported “Yes” (more confidence in calling negative and decreased rate of atypical) 33% reported “No” (hard to strictly follow the algorithm) |
HGUC: High-grade urothelial carcinoma, TPS: The Paris System, NHGUC: Negative for HGUC, AUC: Atypical urothelial cell, LGUN: Low-grade urothelial neoplasm, SHGUC: Suspicious for HGUC, N/C: Nuclear-cytoplasmic, 3D: Three-dimensional
DISCUSSION
The clinical utility of any classification system depends on both its precision (reproducibility) and its diagnostic accuracy. The overall agreement by TPS was fair, with a kappa value of 0.362, which is close to the overall kappa value of 0.32 previously reported by Long et al.[11] TPS demonstrated good precision among NHGUC and HGUC diagnostic categories, whereas other equivocal categories (AUC and SHGUC) demonstrated poor interobserver variability. Similar findings were recently reported by a web-based interobserver study, cosponsored by the American Society of Cytopathology (ASC) and International Academy of Cytology that agreements were highest among the NHGUC and HGUC categories and low in equivocal categories, in concordance with our results.[14] High clinical impact disagreement between the participating cytopathologists occurred in 17% of the study cases, a rate comparable to that recently reported (15%).[11] Both TPS and TM showed comparable sensitivity, specificity, positive and negative predictive values, and accuracy, although TPS showed slightly higher sensitivity and accuracy.
No significant difference in the rate of SHGUC and HGUC categories in both TPS and TM was detected in our study. Differences were significant among the negative and atypical categories. The atypical category has been challenging for both pathologists and clinicians ever since diagnostic systems were designed for reporting urine cytopathology. The definition of the inclusion criteria to use the term “atypical” was often vague and confusing in prior classifications. The frequency of use of the term “atypical” has widely ranged from 2% to 31% in the reported literature. The high frequency of using the atypical category often resulted in over investigation and excessively prolonged surveillance.[15] Furthermore, the risk of urothelial carcinoma associated with the term has varied from 8.3% to 37.5%, a wide range of variation that has only rendered this category almost clinically meaningless.[15161718192021]
An important goal for TPS was to limit the use of AUC diagnosis to cells with atypical features that are more likely to be associated with HGUC. Our results show that TPS is successful in reducing the atypical category. We observed a significant decrease in the rate of atypical diagnosis using TPS (23%) as compared to TM (44%). Recently, published studies have reported TPS AUC rates varying from 22 to 31%.[5111722] In our study, there is a significant difference in the rate of atypical diagnosis after applying TPS, where a total of 64% (28/44) of the cases that were diagnosed as “atypical cells present” by TM were then reclassified as NHGUC by TPS. In other words, TPS has decreased the rate of atypical diagnosis in benign samples by 28%. The reduction in our AUC diagnosis was associated with a significant increase in the rate of NHGUC (54% by TPS vs. 26% by TM). Survey of the study participants suggested that this resulted from the application of well-defined criteria and the change in the terminology from “negative for malignant cells” to the more specific terminology of “negative for HGUC,” thus decreasing the apprehension of missing low-grade carcinoma. In addition, the recommendation to diagnose samples with clusters of small cells and tissue fragments as negative, if no nuclear atypia is present by TPS, also helped reduce the AUC diagnosis. This shift from the AUC category to the NHGUC has also been observed in other studies.[52324252627] Recently published studies have shown that PPV of the AUC category for HGUC has increased after applying TPS (43%–83% in one study and 28%–46% in another).[2325] In our study, the PPV of the AUC category by TPS is 61% (14 of 23 were biopsy-proven HGUC) versus 43% for the atypical category by TM (19 of 44 were biopsy-proven HGUC). In addition, the relative risk (RR) of a sample ending up being biopsy-proven HGUC when called AUC by TPS is twice the risk of it being biopsy-proven non-HGUC when the sample is called NHGUC (RR = 2.054). Therefore, we can conclude that TPS has increased the clinical meaningfulness or the likelihood that the AUC diagnosis represents true HGUC cases. This can eventually result in facilitating clinical decision-making and fewer patients referred to unnecessary cystoscopy procedures, improving the rate of HGUC detection by cystoscopy.[28]
An increased risk of malignancy associated with the NHGUC is observed in our study, where 16 (30%) cases diagnosed as NHGUC by TPS were concurrent biopsy-proven HGUC. Re-review and reclassification of these cases to AUC after observing either rare cells with only slight increase in N/C ratio or focal subtle atypical features in a background of either inflammation, crystals, or degenerative changes resulted in a decrease in risk of malignancy associated with NHGUC category from 30% to 20% (11/54). While 20% risk of malignancy is still high, it has been reported to range from 13% to 37% by other prospective and retrospective studies conducted to evaluate urine samples pre- and post-TPS.[1224] It seems that strictly following the N/C ratio and nuclear hyperchromasia criteria or dismissing subtle atypical features if there is a background of inflammation/degeneration or crystals has resulted in underdiagnosing some of the cases that were biopsy-proven HGUC in this study. This decrease in the detection rate of HGUC after applying TPS was also observed in one other recently published study.[27] We hypothesize that this decrease is the result of three main challenges: the N/C ratio criteria, nuclear hyperchromasia as a required criterion for atypia of high-grade malignancy in the presence of other high-grade criteria, and the less defined guidelines for assessment of samples with degeneration or obscuring inflammatory background/crystals. The clinical impact of decreasing the rate of AUC with a secondary increase in the rate of NHGUC and a potential decrease in the rate of detection of HGUC by TPS needs to be further investigated in large prospective studies.
The diagnostic challenges observed in our study have resulted in an extensive search of the relevant existing published literature. Layfield et al. demonstrated suboptimal interobserver reproducibility of estimated of N/C ratio and Zhang et al. demonstrated that morphologists overestimated the N/C ratio.[2930] A recent study by Cowan et al. found limitations regarding N/C ratio >0.7 and number of cells meeting all HGUC criteria to qualify for this diagnosis, despite improved risk stratification.[3] Another study found that N/C ratio was predictive of malignancy only if observed in single cells, whereas other high-grade criteria such as an irregular nuclear membrane, hyperchromasia, and coarse granular chromatin were predictive in both single cells and groups. Coarse chromatin alone was more specific than other individual features.[42631] Digital image analysis has been shown to support N/C ratio cutoff of 0.5 as a criterion for AUC.[32] A recently published study utilizing digital image analysis found that the average N/C ratio for HGUC was 0.57 and for SHGUC was 0.53, proposing reduction of the N/C ratio criterion to a cutoff below 0.7.[33] HGUC cells have been shown to have different cytologic morphologies, where cells can have atypical or malignant nuclei but with abundant cytoplasm, mimicking umbrella cells, in up to 17% of samples.[34] Finally, degeneration/poor preservation and obscuring inflammation were implicated in 50% of false-negative urine samples.[35] A comprehensive approach to looking at the nuclear criteria proposed by TPS in light of these findings is needed to increase the diagnostic accuracy and detection rate of HGUC.
Hundred percent of the study cases diagnosed as SHGUC by TPS were surgically biopsy-proven HGUC. A similar rate was previously reported in one other study assessing TPS.[36] This raises the question of whether SHGUC should remain a separate category from HGUC. This may also have implications on the interobserver agreement. This prompted re-assessment of interobserver agreement in our study after collapsing the SHGUC and HGUC into one diagnostic category. The overall agreement slightly increased as a result to 0.411. Of note, all samples from our study were collected from the lower urinary tract, where the clinical implication of these two categories might not be as significant as that of samples obtained from the upper urinary tract. Additional large studies with clinical follow-up are needed to further investigate the impact of combining those two categories.
Our end of study survey showed that all cytopathologists agreed that the use of NHGUC terminology proposed by the TPS instead of the general terminology of “negative for malignant cells” traditionally used for that category was quite helpful in focusing on the detection of high-grade lesions. In addition, most of the participating cytopathologists found that the application of TPS was practical and helpful in decreasing the rate of atypical diagnosis, a category that was frequently used as a wastebasket in many cases and has lost its clinical usefulness as a result. Fifty percent found the cell number cutoff of urothelial cells with severe atypia, proposed by TPS as one of the criteria to call HGUC versus SHGUC, helpful. With that said, the overall satisfaction with TPS was 33%, which was mainly attributed to challenges resulting from strictly applying the N/C ratio criteria, especially to differentiate between NHGUC, AUC, and SHGUC, where the N/C ratio differed minimally from the cutoff criteria proposed by TPS. In addition, severe nuclear hyperchromasia and N/C ratio >0.7 as strict requirements to call HGUC were the limiting factors in some cases that met all other criteria listed in those categories. These limitations have resulted in disqualifying some cases that contain overtly malignant cells from HGUC diagnosis.
Our study is limited by the number of cases studied, its retrospective nature, and the fact that only cytology samples with concurrent surgical biopsy were included. Therefore, the reported percentage of each TPS category may not reflect all the cytology samples seen in our laboratory. While we have recently implemented TPS in our laboratory and intend to continue to report on its performance in prospective studies, multiple large prospective studies from different institutions are needed to further refine the diagnostic criteria of TPS, to define the risk related to TPS initial diagnostic categories, and to establish clear-cut clinical management guidelines based on clinical outcomes, with collaborations with urologists to include their valuable feedback.
CONCLUSIONS
The remarkable decrease in the rate of atypical diagnosis and the increased clinical significance of this category as demonstrated in our study is evidence that TPS has improved actionable clinical decision-making. While TPS shows adequate precision for categories NHGUC and HGUC, the interobserver variability for other equivocal categories remains low. Further refinement and widespread application of TPS diagnostic criteria for the atypical and malignant categories may result in higher detection rate of HGUC and improved interobserver agreement.
COMPETING INTERESTS STATEMENT BY ALL AUTHORS
The authors declare that they have no competing interests.
AUTHORSHIP STATEMENT BY ALL AUTHORS
All authors of this article declare that we qualify for authorship as defined by ICMJE.
Each author has participated sufficiently in the work and takes public responsibility.
For appropriate portions of the content of this article, each author acknowledges that this final version was read and approved.
ETHICS STATEMENT BY ALL AUTHORS
This study was conducted with approval from the Institutional Review Board of all the institutions associated with this study as applicable.
LIST OF ABBREVIATIONS (In alphabetic order)
AUC: Atypical urothelial cells
CAP: College of American Pathologists
CI: Confidence intervals
HGUC: High-grade urothelial carcinoma
LGUN: Low-grade urothelial neoplasm
NHGUC: Negative for high-grade urothelial carcinoma
N/C ratio: Nuclear to cytoplasmic ratio
PPV: Positive predictive value
SHGUC: Suspicious for high-grade urothelial carcinoma
TPS: The Paris System
TM: Traditional Method.
EDITORIAL/PEER-REVIEW STATEMENT
To ensure the integrity and highest quality of CytoJournal publications, the review process of this manuscript was conducted under a double-blind model (the authors are blinded for reviewers and vice versa) through automatic online system.
REFERENCES
- The Paris System for reporting urinary cytology: The quest to develop a standardized terminology. Adv Anat Pathol. 2016;23:193-201.
- [Google Scholar]
- The Paris System for reporting urinary cytology improves correlation with surgical pathology biopsy diagnoses of the lower urinary tract. Diagn Cytopathol. 2018;46:221-7.
- [Google Scholar]
- Improved risk stratification for patients with high-grade urothelial carcinoma following application of The Paris System for reporting urinary cytology. Cancer Cytopathol. 2017;125:427-34.
- [Google Scholar]
- Analysis of the cytomorphological features in atypical urine specimens following application of The Paris System for reporting urinary cytology. Acta Cytol. 2018;62:54-61.
- [Google Scholar]
- Impact of implementing The Paris System for reporting urine cytology in the performance of urine cytology a correlative study of 124 cases. Am J Clin Pathol. 2016;146:384-90.
- [Google Scholar]
- Utility of The Paris System in reporting urine cytology. Acta Cytol. 2017;61:145-52.
- [Google Scholar]
- One year of experience using The Paris System for reporting urinary cytology. Cancer Cytopathol. 2018;126:430-6.
- [Google Scholar]
- An institutional experience with The Paris system: A paradigm shift from ambiguous terminology to more objective criteria for reporting urine cytology. Cytopathol. 2017;28:509-15.
- [Google Scholar]
- The Paris system for urine cytology in upper tract urothelial specimens: A comparative analysis with biopsy and surgical resection. Cytopathol. 2018;29:184-8.
- [Google Scholar]
- Applying the Paris system for reporting urine cytology increases the rate of atypical urothelial cells in benign cases: A need for patient management recommendations. Acta Cytol. 2017;61:71-6.
- [Google Scholar]
- Interobserver reproducibility of the Paris system for reporting urinary cytology. Cytojournal. 2017;14:17.
- [Google Scholar]
- The Paris system for reporting urinary cytology: Early review of the literature reveals successes and rare shortcomings. J Am SOc Cytopathol. 2018;7:185-94.
- [Google Scholar]
- Pathogenesis of urothelial carcinoma. In: Rosenthal DL, Wojcik EM, Kurtycz DF, Barkan GA, Pavelec DM, Rosenthal DL, eds. The Paris System for Reporting Urinary Cytology. Switzerland: Springer; 2015. p. :1-4.
- [Google Scholar]
- Diagnostic significance of atypical category in the voided urine samples: A retrospective study in a tertiary care center. Urol Ann. 2010;2:100-6.
- [Google Scholar]
- Accuracy of urine cytology and the significance of an atypical category. Am J Clin Pathol. 2009;132:785-93.
- [Google Scholar]
- The Atypical urothelial cell category in The Paris System: Strengthening the achilles' heel. Cancer Cytopathol. 2016;124:305-6.
- [Google Scholar]
- Diagnostic terminology for urinary cytology reports including the new subcategories 'atypical urothelial cells of undetermined significance' (AUC-US) and 'cannot exclude high grade' (AUC-H) Cytopathology. 2014;25:27-38.
- [Google Scholar]
- Evaluation of atypical urine cytology progression to malignancy. Cancer Cytopathol. 2013;121:387-91.
- [Google Scholar]
- Malignant atypical cell in urine cytology: A diagnostic dilemma. Cytojournal. 2006;3:28.
- [Google Scholar]
- The johns hopkins hospital template for urologic cytology samples Parts II and III – Improving the predictability of indeterminate results in urinary cytologic samples: An outcomes and cytomorphologic study. Cancer Cytopathol. 2013;121:21-8.
- [Google Scholar]
- The Johns Hopkins hospital template for urologic cytology samples Part I-Creating the template. Cancer Cytopathology. 2013;121:15-20.
- [Google Scholar]
- Improved diagnostic precision of urine cytology by implementation of The Paris System and the use of cell blocks. Cancer Cytopathol. 2018;126:809-16.
- [Google Scholar]
- Evaluation of The Paris System in atypical urinary cytology. Cytopathology. 2018;29:545-9.
- [Google Scholar]
- Implementing The Paris System for reporting urinary cytology results in a decrease in the rate of the “atypical” category and an increase in its prediction of subsequent high-grade urothelial carcinoma. Cancer Cytopathol. 2018;126:207-14.
- [Google Scholar]
- Modification of The Paris System for urinary tract washing specimens using diagnostic cytological features. Cytopathol. 2017;28:516-23.
- [Google Scholar]
- Clinical follow up and the impact of The Paris System in the assessment of patients with atypical urine cytology. Diagn Cytopathol. 2018;46:1022-30.
- [Google Scholar]
- Urinary cytology and The Paris System for reporting urinary cytology: Implications for urological management. Cytopathol. 2018;29:368-70.
- [Google Scholar]
- Accuracy and Reproducibility of Nuclear/Cytoplasmic Ratio Assessments in Urinary Cytology Specimens. Diagn Cytopathol. 2017;45:107-12.
- [Google Scholar]
- Morphologists overestimate the nuclear-to-cytoplasmic ratio. Cancer Cytopathol. 2016;124:669-77.
- [Google Scholar]
- Hypochromatic large urothelial cells in urine cytology are indicative of high grade urothelial carcinoma. APMIS. 2018;126:705-9.
- [Google Scholar]
- Digital image analysis supports a nuclear-to-cytoplasmic ratio cutoff value of 0.5 for atypical urothelial cells. Cancer Cytopathol. 2017;125:710-6.
- [Google Scholar]
- Digital image analysis supports a nuclear-to-cytoplasmic ratio cutoff value below 0.7 for positive for high-grade urothelial carcinoma and suspicious for high-grade urothelial carcinoma in urine cytology specimens. Cancer Cytopathol. 2019;127:120-4.
- [Google Scholar]
- High-Grade urothelial carcinoma on urine cytology resembling umbrella cells. Acta Cytol. 2018;62:62-7.
- [Google Scholar]
- Causes of false-negative for high-grade urothelial carcinoma in urine cytology. Diagn Cytopathol. 2016;44:994-9.
- [Google Scholar]
- Application of The Paris System to atypical urine cytology samples: Correlation with histology and UroVysion (R) FISH. Cytopathol. 2017;28:88-95.
- [Google Scholar]




