


Translate this page into:
Role of immunocytochemistry in cervical cancer screening

*Corresponding author: Vinod B. Shidham, MD,FIAC,FRCPath, Department of Pathology, Wayne State University School of Medicine, Karmanos Cancer Center and Detroit Medical Center, Detroit, Michigan, United States. vshidham@med.wayne.edu
-
Received: ,
Accepted: ,
How to cite this article: Shidham VB. Role of immunocytochemistry in cervical cancer screening. CytoJournal 2022;19:42.
Abstract
The cervical cancer screening has been based conventionally on cytologic analysis. With advances in understanding the role of human papillomavirus, cotesting has been applied. But most of the patients subjected to colposcopy did not benefit, except in cases with HSIL [high-grade squamous intraepithelial lesion] cytology. Because of this, a step to increase the sensitivity to detect cancers and pre-cancers but with higher specificity with minimal overdiagnosis leading to prevention of unindicated cervical biopsies is highly desired. Such triaging step in cases with abnormal screening results is expected to minimize invasive interventions because of low false positivity. With availability of methodologies leading to quantitatively and qualitatively enhanced cell-blocks from residual liquid based cytology specimens, immunostaining can be performed for multiple immunomarkers with potential objectivity to triage initial screening test results. This is enhanced further with inclusion of AV marker in the cell-blocks and application of SCIP (subtractive coordinate immunoreactivity pattern) approach. The cell-blocks are also resource for performing other ancillary studies including molecular pathology and proteomics/metabolomics as potential tests in future. This review explores application of residual liquid based cytology specimen for cell-blocking with application of ancillary studies in algorithmic manner as adjunct to ASCCP management guidelines for improved patient care.
Keywords
Cervical cancer
PAP test
Papanicolaou smear
Cell-block
Liquid based cytology
LBC
Immunohistochemistry
Immunocytochemistry
Cervical cytology
HPV
p16
Ki-67

Conventionally, primary screening for cervical cancer was based on cytologic analysis. With our growing understanding of role of human papillomavirus (HPV) in cervical cancer and advent of HPV testing, the sensitivity for detecting cervical intraepithelial neoplasia (CIN) 2 and worse lesions has improved. However, this has resulted in overdiagnosis and treatment of HPV infection, because the lifetime risk of having HPV is high (90%). However, the fact is that most HPV infections (80%) will clear within 2 years.
Studies have shown that with cotesting (simultaneous cytology and high-risk HPV [hrHPV] deoxyribonucleic acid [DNA] testing), 60–80% of patients who underwent colposcopy did not benefit (except for those reported as high-grade squamous intraepithelial lesion [HSIL] by cytology).
This clearly indicates that there should be a step which not only increases the sensitivity to detect cancers and pre-cancers but also achieves higher specificity by reducing overdiagnoses and unnecessary invasive interventions during cervical cancer screening. Therefore, there is a need to triage patients with abnormal screening results for minimizing the number of false positives.
ABNORMAL SCREENING RESULTS: IMMUNOSTAINING AS TRIAGE?
Liquid-based cytology (LBC) has opened up the option to apply immunocytochemical (ICC) testing of cervical cells. ICC is being used as a method of triage and screening, using several newly discovered immunomarkers associated with the development of cervical cancer and pre-cancer.
Other less appreciated insight is that the cervical cytology specimens are equivalent to brush biopsy with singly scattered epithelial cells and some microfragments from squamocolumnar area at the junction of ectocervix and endocervix. If these cells could be properly cell-blocked and cut similar to surgical biopsy, then the sections could be subjected to immunohistochemical testing and other ancillary studies.
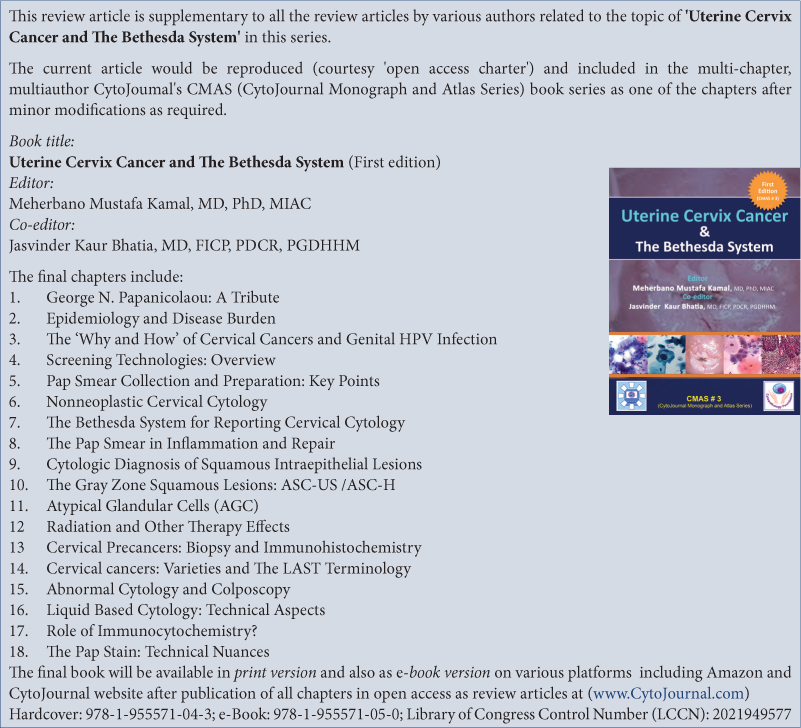
Recently, Shidham cell-blocking method with AV marker to monitor the depth of cutting for preventing the loss of diagnostic cells while section cutting is reported to make cell-blocks from LCB [Figure 1].[1] Immunostaining performed on the sections of these cell-blocks has reported evaluation of p16INK4a (p16) with good results on SurePath LBC specimens.[2-4] However, this method is difficult to be organized and practiced from scratch at individual laboratory level. Lately, easy and ready to use cell-blocking kits based on this method are available with quantitative and qualitative enhancements in cell-blocking.[5-9] These cell-blocks prepared with Nano NextGen CelBloking™ kits with built-in AV marker allow easy application of subtractive coordinate immunoreactivity pattern (SCIP) approach for the evaluation of coordinate immunoreactivity for multiple immunomarkers in serial sections.[8] In addition, these cell-blocks may also be used for application of other ancillary studies including molecular pathology and proteomics/ metabolomics.[9-12]
![Comparison of cellularity of sections of cell-block with and without AV marker. (Reproduced under Open-Access charter from: Varsegi GM, Shidham V. J Vis Exp 2009;29:1316. doi: 10.3791/1316).[1]](/content/105/2022/19/1/img/Cytojournal-19-42-g001.png)
- Comparison of cellularity of sections of cell-block with and without AV marker. (Reproduced under Open-Access charter from: Varsegi GM, Shidham V. J Vis Exp 2009;29:1316. doi: 10.3791/1316).[1]
Routine chromogenic immunostaining for p16 with light microscopy can be performed on LBC preparations.[13] However, immunostained cytology preparations would not allow coordinate evaluation of multiple immunomarkers on the same cells in a fashion comparable to that achieved in serial sections of cell-block.[8]
Based on this, it is obvious that the LBC is a significant noninvasive sampling resource as brush biopsy. The residual specimen may be subjected to cell-blocking as indicated. An algorithm [Figures 2 and 3] suggested in this chapter may be applied for maximum outcome from LBC specimen to minimize the need for additional invasive interventions with profound benefits in terms of cost containment with improved patient care [Figure 4] as adjunct to ASCCP management guidelines.[14]
![Algorithm showing cases which may be triaged to make cell-block from residual liquid-based cytology specimens with enhanced methods such as with Nano NextGen CelBloking™ kits.[5] LG: Low grade, HG: High grade, HPV: Human papillomavirus.](/content/105/2022/19/1/img/Cytojournal-19-42-g002.png)
- Algorithm showing cases which may be triaged to make cell-block from residual liquid-based cytology specimens with enhanced methods such as with Nano NextGen CelBloking™ kits.[5] LG: Low grade, HG: High grade, HPV: Human papillomavirus.
![Algorithm showing application of immunostaining cell-block sections with subtractive coordinate immunoreactivity pattern. The evaluation may be refined further using digital imaging methodologies and application of high-dimensional imaging of multiplexed ion beam imaging by time-of-flight.[31] AGC: Atypical glandular cells, AIS: Adenocarcinoma in situ, AdCa: Adenocarcinoma. *May also be used for Molecular pathology studies including miRNA testing and proteomics **Depending on clinical scenario including known history of cancer, imaging findings etc](/content/105/2022/19/1/img/Cytojournal-19-42-g003.png)
- Algorithm showing application of immunostaining cell-block sections with subtractive coordinate immunoreactivity pattern. The evaluation may be refined further using digital imaging methodologies and application of high-dimensional imaging of multiplexed ion beam imaging by time-of-flight.[31] AGC: Atypical glandular cells, AIS: Adenocarcinoma in situ, AdCa: Adenocarcinoma.
- *May also be used for Molecular pathology studies including miRNA testing and proteomics
- **Depending on clinical scenario including known history of cancer, imaging findings etc
![Interpretation of immunostaining with subtractive coordinate immunoreactivity pattern approach for definitive management. The evaluation may be refined further using digital imaging methodologies and application of high-dimensional imaging of multiplexed ion beam imaging by time-of-flight.[31]](/content/105/2022/19/1/img/Cytojournal-19-42-g004.png)
- Interpretation of immunostaining with subtractive coordinate immunoreactivity pattern approach for definitive management. The evaluation may be refined further using digital imaging methodologies and application of high-dimensional imaging of multiplexed ion beam imaging by time-of-flight.[31]
Better recommendation is to collect routine LBC specimen in LBC collection vial followed by dedicated sampling from transformation zone which may be collected with more pressure for deeper sampling. This should be submitted directly in 10% formalin for cell-blocking with enhancement methods such as Nano NextGen CelBloking™ kits. These cell-blocks can be used to apply the algorithm recommended in [Figures 2 and 3]. Because these are equivalent to dedicated brush biopsy of transformation zone, it would be a quantitative and qualitative improvement with higher positive predictive value (PPV).
IMMUNOMARKERS WHICH WOULD IMPROVE THE ACCURACY OF CERVICAL CANCER SCREENING AND REDUCE UNNECESSARY INVASIVE EXAMINATIONS [Figures 2 and 3]
Cervical squamous lesions:
p16 with Ki 67
Other immunomarkers: ProEx
Glandular lesions:
Endocervical: p16 with Ki-67, mCEA[15]
Endometrial: Vimentin+,[16] PAX8 +,[17] Ki-67[18]
Ovarian: Vimentin –,[16] PAX8 +,[17] Ki-67[18]
Other metastasis:
Immunomarkers specific for the primary site.[8]
Currently, commonly applied immunomarkers include p16, Ki-67, and ProExC in various combinations. p16 and ProExC are both markers related to aberrant cell cycle due to the oncogenic effects of HPV. Ki-67 is immunomarker for cellular proliferation.
p16 IN CERVICAL CANCER
The cyclin-dependent protein kinase inhibitor p16 is a negative regulator of the cell cycle pathway of cyclinDCDK4/6-pRb-E2F that regulates the transition from the G1 to the S phase of the cell cycle and normally functions as a cell cycle brake through inhibitory effects of Rb gene.[19,20] In cervical HSIL and carcinomas, induced by persistent infection by hrHPV, the E7 viral oncoprotein binds to the host Rb protein (pRb). This results in the functional inactivation of retinoblastoma protein.[21] This leads to the overexpression of p16 gene with increased production of the p16 (from negative transcriptional feedback control).
Ki-67
Ki-67 is a nuclear antigen expressed in all phases of the cell cycle except for G0 phase and is a proliferation marker.[18] Functional inactivation of pRb may lead to genetic instability in normal cells; however, it will cause malignant transformation in DNA replication in the competent cells. Therefore, simultaneous detection of tumor suppressor gene p16 overexpression as nuclear immunoreactivity and nuclear immunoexpression of the proliferation marker Ki-67 within the same cervical epithelial cell should indicate deregulation of the cell cycle and equate with high-grade lesions, which is independent of morphological examination results. Because in normal cells, p16 functions as a tumor suppressor gene and the Ki-67 functions as a cellular proliferation marker, they should be mutually exclusive and are not expressed simultaneously.
DUAL IMMUNOSTAINING WITH p16/Ki-67[Figure 5]
Application of p16 immunocytochemistry alone was studied initially in cervical cytology samples.[2,13] Although the results were promising for predicting the risk of HSIL, occasional staining of non-HSIL cells has been problematic. Same challenge may also be applicable to cervical biopsies. However, in contrast to cytology preparations, biopsy allows evaluation of architectural details which facilitates appropriate interpretation of immunoreactivity in non-HSIL cells including some reactive/ non-neoplastic cells such as tubal metaplasia as non-diagnostic.
![p16/Ki-67 dual-staining positive cells with morphological features of HSIL. (a) Liquid-based cytology (SurePath). (b) Slide A was dual stained with p16/Ki-67. Cell with p16 staining alone (blue arrow) is characterized by a brown cytoplasmic/nuclear signal and cell with Ki-67 staining alone (red arrow) is presented in red nuclear signal. The positive p16/Ki-67 dual-staining cells (dark arrow) are characterized by a brown cytoplasmic signal for p16 overexpression and a dark red nuclear signal for p16/Ki-67 coexpression in the same cell (a 45-year-old woman, CIN3, HPV16+, p16/Ki-67+). (Reproduced from open-access publication: Yu L et al. J Cancer 2019;10:2654-60. doi:10.7150/jca.32743).[23]](/content/105/2022/19/1/img/Cytojournal-19-42-g005.png)
- p16/Ki-67 dual-staining positive cells with morphological features of HSIL. (a) Liquid-based cytology (SurePath). (b) Slide A was dual stained with p16/Ki-67. Cell with p16 staining alone (blue arrow) is characterized by a brown cytoplasmic/nuclear signal and cell with Ki-67 staining alone (red arrow) is presented in red nuclear signal. The positive p16/Ki-67 dual-staining cells (dark arrow) are characterized by a brown cytoplasmic signal for p16 overexpression and a dark red nuclear signal for p16/Ki-67 coexpression in the same cell (a 45-year-old woman, CIN3, HPV16+, p16/Ki-67+). (Reproduced from open-access publication: Yu L et al. J Cancer 2019;10:2654-60. doi:10.7150/jca.32743).[23]
In cytologic samples without architectural reference points, concurrent application of Ki-67 immunostaining (a marker of cycling cells) facilitates confirmation of p16 immunoreactivity in abnormal cells. It is claimed that p16/Ki-67 dual immunostaining increases sensitivity and specificity for detecting cervical pre-cancer than other immunostaining approach in cytology preparation. This could effectively reduce the unindicated colposcopy and invasive interventions.[22,23]
hrHPV infection-related deregulation of the cell cycle predicts high-grade cervical epithelial lesion. p16/Ki-67 dual immunostaining of cytology preparation has been recommended as biomarker with higher PPV.[23-27] However, because both p16 and Ki-67 are nuclear immunostain, their concomitant immunoreactivity even with two different colors would be challenging to interpret. Because of this, it is difficult to interpret the results.[23] This is especially difficult in cases with strong intensity of brown immunostaining for nuclear p16 which could potentially mask the concomitant red Ki-67 nuclear immunoreactivity.[24] Depending on quantitative and qualitative factors, in these cases, there may be some cells with distinct dual immunostaining.
Automated evaluation with digital analysis of p16/Ki-67 dual immunostained is reported.[25] It is surprising to note that some reports[26] consider p16 cytoplasmic immunoreactivity as diagnostic for HPV-related phenomenon to be interpreted as positive and then concurrent nuclear Ki-67 immunoreactivity is easy to interpret. However, this approach has basic flaw due to dependance on cytoplasmic p16 immunoreactivity as HPV related phenomenon.
PALMS STUDY: p16/Ki67 DUAL STAINING IN ASCUS/LSIL ON CYTOLOGY PREPARATIONS[28]
The results showed that PPV was higher in CIN2+ for dual-immunostained cytology as compared to HC2 HPV testing. This is also true for cases with LSIL and ASC-US, especially in women <30 years.[28] This pan-European prospective study showed that dual-stained cytology showed high PPV to help minimize the number of unindicated colposcopy referrals and invasive interventions.
It has been suggested that dual-stained cytology screening may play a role in younger women where hrHPV testing has limitations. A health economic analysis also should be performed to assess the cost-effectiveness and economic impact of this triage strategy, particularly for its use in developing countries.
OTHER BIOLOGICAL MARKERS
ProExC in cervical cancer
Minichromosome maintenance protein 2 (MCM2) and topoisomerase II-α (TOP2A) are two biomarkers that are involved in DNA replication. MCM2 protein is associated with G1 phase of the cell cycle and DNA synthesis with helicase activity for DNA unwinding. During replication, TOP2A enzyme is related to unlinking DNA strands. Expressions of these genes are increased in cervical carcinoma. ProEx C (BD Diagnostics-Tripath, Burlington, NC) is a new immunomarker which includes monoclonal antibodies to TOP2A and MCM2, respectively.[29,30] BD ProEx™ C ProExC [Figure 6] has shown utility in the triage of atypical glandular cells and ASC-H and as a follow-up ICC test after primary HPV screening.
![Left: A case interpreted as LSIL (Pap, ×200); Right: Nuclear ProExC immunostaining in the same case (ProExC, ×100). (Reproduced from open-access publication: Tosuner Z et al. J Cytol 2017;34:34-8. doi:10.4103/0970-9371.197605).[29]](/content/105/2022/19/1/img/Cytojournal-19-42-g006.png)
- Left: A case interpreted as LSIL (Pap, ×200); Right: Nuclear ProExC immunostaining in the same case (ProExC, ×100). (Reproduced from open-access publication: Tosuner Z et al. J Cytol 2017;34:34-8. doi:10.4103/0970-9371.197605).[29]
Other markers include HPV L1 capsid protein, claudin 1, BCL2-associated X/BCL2 antagonist/killer (Bax/Bak), insulin-like growth factor-II mRNA-binding protein 3 (IMP3), Mindbomb E3 ubiquitin protein ligase 1 (MIB1), Raf kinase inhibitor Protein, and Feulgen-thionin staining.[19]
FUTURE PROGRESS
Immunostaining of the sections of cell-block from residual cervical LBC samples would overcome the difficulty associated with interpretation of dual color p16/Ki-67 immunostaining with more objectivity. This would increase the PPV for the detection of HSIL and higher lesions in sections of cell-block from residual LBC specimen equivalent to brush biopsy with the results comparable to surgical biopsies.
The residual LBC specimens can be cell-blocked with utilization of entire sampled material equivalent to brush biopsy [Figures 7-9].[1-7,13] The cell-block sections could be stained with SCIP approach on adjacent serial sections for reliable evaluation of nuclear immunoreactivity for p16 and Ki-67 in the same cells with morphological evaluation of same cells on HE section in SCIP sections.[8] Other immunomarkers and chromogenic in situ hybridization (CISH) may be performed on additional sections.[9] For improved objectivity, the serial level sections with SCIP approach could be digitized and precisely superimposed for improved and rapid interpretation.
Other future option would be to apply high-dimensional imaging of multiplexed ion beam imaging by time-of-flight as a form of mass spectrometry (MS) imaging. The metal labeled antibodies and secondary ion MS are performed on the same tissue section to image different proteins simultaneously for multiplexed immunohistochemistry approaches.[31]
![(a) Pap smear interpreted as LSIL, (b) H and E cell-block sections, (c) p16-stained cell-block sections, and (d) biopsy showing CIN II-III. (Reproduced under open-access charter from: Shidham VB et al. CytoJournal 2011;8:1).[4]](/content/105/2022/19/1/img/Cytojournal-19-42-g007.png)
- (a) Pap smear interpreted as LSIL, (b) H and E cell-block sections, (c) p16-stained cell-block sections, and (d) biopsy showing CIN II-III. (Reproduced under open-access charter from: Shidham VB et al. CytoJournal 2011;8:1).[4]
![(a) ASC-H (rare single cells with hyperchromatic nuclei and high N: C ratios), (b) H and E stained cell-block sections, (c) p16-stained sections highlighting scattered high-grade cells, and (d) biopsy showing CIN III with extensive endocervical glandular involvement. (Reproduced under open-access charter from: Shidham et al. CytoJournal 2011;8:1).[4]](/content/105/2022/19/1/img/Cytojournal-19-42-g008.png)
- (a) ASC-H (rare single cells with hyperchromatic nuclei and high N: C ratios), (b) H and E stained cell-block sections, (c) p16-stained sections highlighting scattered high-grade cells, and (d) biopsy showing CIN III with extensive endocervical glandular involvement. (Reproduced under open-access charter from: Shidham et al. CytoJournal 2011;8:1).[4]
![(a) Pap smear interpreted HSIL, (b) H and E cell-block section containing “microbiopsies,” (c) p16-stained cell-block section showing true nuclear immunoreactivity, and (d) biopsy showing invasive squamous cell carcinoma. (Reproduced under open-access charter from: Shidham VB et al. CytoJournal 2011;8:1).[4]](/content/105/2022/19/1/img/Cytojournal-19-42-g009.png)
- (a) Pap smear interpreted HSIL, (b) H and E cell-block section containing “microbiopsies,” (c) p16-stained cell-block section showing true nuclear immunoreactivity, and (d) biopsy showing invasive squamous cell carcinoma. (Reproduced under open-access charter from: Shidham VB et al. CytoJournal 2011;8:1).[4]
miRNA AND CERVICAL CANCER[32] [Figures 10 and 11]
microRNAs (miRNAs) are major players in post-transcriptional gene regulation and are small, non-coding RNAs involved in all processes ranging from carcinogenesis to viral infection responses. In contrast to most RNAs, miRNA is relatively stable and so is relatively easy to study under laboratory conditions.[33]
![miRNAs and cervical neoplasia progression. Reproduced from open-access publication: Pardini B et al. BMC Cancer 2018;18:696. 10.1186/s12885-018-4590-4 .[38]](/content/105/2022/19/1/img/Cytojournal-19-42-g010.png)
- miRNAs and cervical neoplasia progression. Reproduced from open-access publication: Pardini B et al. BMC Cancer 2018;18:696. 10.1186/s12885-018-4590-4 .[38]
![Differential expression of miRNA in exfoliative cytology of cervical lesions with diagnostic accuracy (modified from[32]). *Six miRNAs (miR-424, miR-375, miR-34a, miR-218, miR-92a, and miR-93). Bold-Trials with the best diagnostic performance. LSIL: Low-grade squamous intraepithelial lesion (milder than CIN2), HSIL: High-grade squamous intraepithelial lesion (CIN2, CIN3, and CIS), AUC: Area under the ROC (receiver operating characteristic) curve, Sn: Sensitivity, Sp: Specificity.](/content/105/2022/19/1/img/Cytojournal-19-42-g011.png)
- Differential expression of miRNA in exfoliative cytology of cervical lesions with diagnostic accuracy (modified from[32]). *Six miRNAs (miR-424, miR-375, miR-34a, miR-218, miR-92a, and miR-93). Bold-Trials with the best diagnostic performance. LSIL: Low-grade squamous intraepithelial lesion (milder than CIN2), HSIL: High-grade squamous intraepithelial lesion (CIN2, CIN3, and CIS), AUC: Area under the ROC (receiver operating characteristic) curve, Sn: Sensitivity, Sp: Specificity.
hrHPV infection associated with cervical cancer are also involved with various miRNAs, which could be applied as biomarker in the management of cervical cancer from screening to the selection of therapy choices. miRNAs may be applied for personalized diagnostics in this area. Metadata analysis suggests high sensitivity and specificity related to cervical cancer. However, due to lack of standardization of methodology and relatively new status, various molecular tools and methodologies are required to be studied to refine the diagnostic and prognostic applications of miRNAs.
Because miRNA is relatively stable as formalin-fixed paraffin-embedded tissue,[33] it can be analyzed as in situ studies[34-37] with CISH methodology and interpretation approach comparable to that for immunostaining. Based on this, various miRNAs associated with different stages of cervical cancer may be tested on cell-block sections with benefits of morphological feedback.
miRNAs reported by various studies in relation to normal cytology and various types of abnormal cytology including milder than CIN2 and severe than CIN2 are summarized in Figures 10 and 11.[32-34,38-42] However, methodologies and techniques related to various steps in the analysis of miRNA should be standardized for proper reproducible results.
miRNA expression levels depend on the stage of cervical pathology with biological fluctuations and show statistically significant variation only in advanced cervical cancer.[32] Similarly, some miRNA expression may represent earlier stage which is not expressed yet morphologically as cytological/histological changes. Ongoing research would be a significant advantage, leading to emergence of novel miRNA candidates for objective testing modality with higher PPV.
The pattern of miRNA expression is dependent on multiple factors. As applicable to other biomarkers, only one miRNA as a perfect marker is suboptimal approach. Most appropriate strategy would be to generate a battery of miRNA as a signature [Figure 10] which will maximize the PPV. miRNA profile may be evaluated on the sections of cell-block prepared from the residual cytology specimen with exfoliated cells as brush biopsy collected noninvasively in the LBC medium. The number of miRNAs to be included, if CISH approach is selected, have to be relatively few with at least two negatives and two positive miRNA candidates for a particular diagnostic category [Figure 11].
In addition, molecular features of cervical cancer may vary because it is not a single disease. In the future, additional spectrums of miRNA patterns may add to the personalized approach in diagnostic and prognostic testing.
PROTEOMICS AND TISSUE-BASED METABOLOMICS [Figure 12]
Proteomics is the study of proteome which includes all proteins produced after alternative splicing and post-translational modifications[9-11] facilitating comprehensive insight into the biological system under evaluation. It includes evaluation of various features related to characterization, quantitative protein expression, protein turnover, degradation, stability, structure, and function. In addition, it also studies post-translational modifications, migration, and protein-protein interaction.
![The workflow in proteomic studies in cervical cancer. This facilitates search for biomarkers that could be applied in the management of cervical cancers from diagnosis to application of new therapeutic targets. The steps include: (1) Biological samples from patients in various forms including FFPE of cell-blocks of cervical specimens are processed to lyse the cells mechanically. (2) Purification of total proteins. (3) The storage at −20°C or −70°C (with or without protease inhibitor) depending on the method selected for proteomic analysis (to avoid any interference). (4) Selection of advanced techniques such as protein microarray, mass spectrometry, 2D gel, 2D-DIGE, and Edman sequencing; quantitative techniques such as ICAT, SILAC, and iTRAQ; high-throughput techniques such as X-ray crystallography and NMR spectroscopy. (5) Analysis with databases and validation of candidate biomarkers by ELISA, western blot, or immunohistochemistry. (Reproduced after minor modification from open-access publication: Martínez-Rodríguez F et al. Cells 2021;10:1854. 10.3390/cells10081854 .[10]](/content/105/2022/19/1/img/Cytojournal-19-42-g012.png)
- The workflow in proteomic studies in cervical cancer. This facilitates search for biomarkers that could be applied in the management of cervical cancers from diagnosis to application of new therapeutic targets. The steps include: (1) Biological samples from patients in various forms including FFPE of cell-blocks of cervical specimens are processed to lyse the cells mechanically. (2) Purification of total proteins. (3) The storage at −20°C or −70°C (with or without protease inhibitor) depending on the method selected for proteomic analysis (to avoid any interference). (4) Selection of advanced techniques such as protein microarray, mass spectrometry, 2D gel, 2D-DIGE, and Edman sequencing; quantitative techniques such as ICAT, SILAC, and iTRAQ; high-throughput techniques such as X-ray crystallography and NMR spectroscopy. (5) Analysis with databases and validation of candidate biomarkers by ELISA, western blot, or immunohistochemistry. (Reproduced after minor modification from open-access publication: Martínez-Rodríguez F et al. Cells 2021;10:1854. 10.3390/cells10081854 .[10]
Application of high-throughput techniques to the biological samples such as cervical cytology specimens, including the cell-blocks prepared from it, allows analyzing cluster of differential molecular profiles related to the genome, the transcriptome, or the proteome. This analysis may generate molecular signature(s) of a particular cancer including different grades of CIN and cervical cancer. In addition to diagnostic and therapeutic contributions, it also assists in elucidation of the pathways related to the development and progression of cancer. This may assist in detecting cervical cancer in its early stages with improvement in survival rate, prognosis, and recurrence.[10]
The analytical techniques may include 1D SDS-PAGE gels, western blot, or ELISA, which may not allow analysis of proteins on massive scale. However, these methods provide access to lot of valuable information for validation studies to check the data generated by MS or two-dimensional gels electrophoresis (2-DE). Ultimately, many of these biomarkers identified with proteomic studies can be applied in routine clinical practice as immunomarkers for immunostaining of cell-block sections.
Metabolomics is the large-scale study of small molecules of metabolites in tissues including their interactions as metabolome. Studies on cervical specimens showed metabolomics typical for cervical carcinoma and HPV infection with potential to be biomarkers for these pathologies.[12] Metabolomics profile showed decreased α- and β-glucose with increased lactate and low-density lipoproteins with altered expression of multiple amino acids. There was a significant increase in transcript and protein levels of glycogen synthase kinase 3 beta and glutamate decarboxylase 1 with drop in transcript and protein levels of pyruvate kinase muscle isoenzyme 2 and carnitine palmitoyltransferase 1A. These features may be used in the future for detecting HPV infection and diagnosing cervical cancers by analyzing aberrant regulation of enzymes associated with metabolic pathways.
Acknowledgment
The authors thank Janavi Kolpekwar for her copy-editing support.
LIST OF ABBREVIATIONS (In alphabetic order)
ASCUS – Atypical squamous cells of undetermined significance
CIN – Cervical intraepithelial neoplasia
CISH – Chromogenic in situ hybridization
DNA – Deoxyribonucleic acid
FDA – Food and Drug Administration
HC – Hybrid capture
HPV – Human papillomavirus
hrHPV – High-risk
HPV HSIL – High-grade squamous intraepithelial lesion
ICC – Immunocytochemical
LBC – Liquid-based cytology
LSIL – Low-grade squamous intraepithelial lesions
miRNAs – microRNAs p16 – p16INK4a
PPV – Positive predictive values
RNA – Ribonucleic acid
SCIP – Subtractive coordinate immunoreactivity pattern
References
- Cell block preparation from cytology specimen with predominance of individually scattered cells. J Vis Exp. 2009;29:1316.
- [CrossRef] [Google Scholar]
- p16INK4a Immunocyto-chemistry as an adjunct to cervical cytology potential reflex testing on specially prepared cellblocks from residual liquid based cytology (LBC) specimens. Mod Pathol. 2009;22(Suppl 1):97.
- [Google Scholar]
- Objective and definitive subcategorization of LSIL with p16INK4a immunocytochemistry on cell block sections of cervical cytology specimens. Cancer Cytopathol. 2009;117:349-450.
- [Google Scholar]
- p16 INK4a immunocytochemistry on cell blocks as an adjunct to cervical cytology: Potential reflex testing on specially prepared cell blocks from residual liquid-based cytology specimens. CytoJournal. 2011;8:1.
- [CrossRef] [PubMed] [Google Scholar]
- NextGen CelBlokingTM kits. AV BioInnovation. Available from: https://www.avbioinnovation.com [Last accessed on 2022 Apr 26]
- [Google Scholar]
- Demo Video: Nano: NextGen CelBlokingTM kits. Available from: https://youtube/y29SS1NwO_8 [Last accessed on 2022 Apr 26]
- [Google Scholar]
- Demo Video: Micro: NextGen CelBlokingTM kits. Available from: https://youtube/i-ZpXaljiIs [Last accessed on 2022 Apr 26]
- [Google Scholar]
- Cell-blocks and other ancillary studies (including molecular pathology and proteomics) Cytojournal. 2021;18:4.
- [CrossRef] [PubMed] [Google Scholar]
- Understanding cervical cancer through proteomics. Cells. 2021;10:1854.
- [CrossRef] [PubMed] [Google Scholar]
- Quantitative proteomic analysis of cervical cancer based on TMT-labeled quantitative proteomics. J Proteomics. 2022;252:104453.
- [CrossRef] [PubMed] [Google Scholar]
- Tissue-based metabolomics reveals potential biomarkers for cervical carcinoma and HPV infection. Bosn J Basic Med Sci. 2020;20:78-87.
- [CrossRef] [PubMed] [Google Scholar]
- Human papilloma virus testing and p16 immunohistochemistry as ancillary/reflex tests in ASC-H cervical-vaginal cytology. Mod Pathol. 2013;26(Suppl 2):98A.
- [Google Scholar]
- 2019 ASCCP risk-based management consensus guidelines for abnormal cervical cancer screening tests and cancer precursors. J Low Genit Tract Dis. 2020;24:102-31.
- [CrossRef] [PubMed] [Google Scholar]
- Cervical cytology and immunohistochemical features in a case of endometrial adenocarcinoma simulating microglandular hyperplasia. Acta Cytol. 2000;44:661-6.
- [CrossRef] [PubMed] [Google Scholar]
- Differential vimentin expression in ovarian and uterine corpus endometrioid adenocarcinomas: Diagnostic utility in distinguishing double primaries from metastatic tumors. Int J Gynecol Pathol. 2014;33:274-81.
- [CrossRef] [PubMed] [Google Scholar]
- PAX8. Available from: https://www.pathologyoutlines.com/topic/stainspax8.html [Last accessed on 2022 Apr 04]
- [Google Scholar]
- Ki-67: More than a proliferation marker. Chromosoma. 2018;127:175-86.
- [CrossRef] [PubMed] [Google Scholar]
- Progress in immunocytochemical staining for cervical cancer screening. Cancer Manag Res. 2019;11:1817-27.
- [CrossRef] [PubMed] [Google Scholar]
- Use of immunohistochemical staining for p16 in gynecological cytology. Cancer Cytopathol. 2016;124:611-2.
- [CrossRef] [PubMed] [Google Scholar]
- Neoplasia In: Kumar V, Abbas AK, Aster JC, eds. Robbins Basic Pathology (10th ed). Philadelphia, PA: Elsevier; 2018. p. :189-242.
- [Google Scholar]
- Role of p16/Ki-67 dual immunostaining in detection of cervical cancer precursors. J Cytol. 2018;35:153.
- [CrossRef] [PubMed] [Google Scholar]
- Application of p16/ Ki-67 dual-staining cytology in cervical cancers. J Cancer. 2019;10:2654-60.
- [CrossRef] [PubMed] [Google Scholar]
- Immunocytochemical colocalization of P16(INK4a) and Ki-67 predicts CIN2/3 and AIS/adenocarcinoma. Cancer Cytopathol. 2012;120:26-34.
- [CrossRef] [PubMed] [Google Scholar]
- Semantic focusing allows fully automated single-layer slide scanning of cervical cytology slides. PLoS One. 2013;8:e61441.
- [CrossRef] [PubMed] [Google Scholar]
- Triage of LSIL/ASC-US with p16/Ki-67 dual staining and human papillomavirus testing: A 2-year prospective study. Cytopathology. 2016;27:269-76.
- [CrossRef] [PubMed] [Google Scholar]
- p16/Ki-67 dual staining has a better accuracy than human papillomavirus (HPV) testing in women with abnormal cytology under 30 years old. Bosn J Basic Med Sci. 2019;19:336-41.
- [CrossRef] [PubMed] [Google Scholar]
- Prospective evaluation of p16/Ki-67 dual-stained cytology for managing women with abnormal Papanicolaou cytology: PALMS study results. Cancer Cytopathol. 2015;123:373-81.
- [CrossRef] [PubMed] [Google Scholar]
- Immunocytoexpression profile of ProExC in smears interpreted as ASC-US, ASC-H, and cervical intraepithelial lesion. J Cytol. 2017;34:34-8.
- [CrossRef] [PubMed] [Google Scholar]
- Detecting high-grade cervical disease on ASC-H cytology: Role of BD ProEx C and Digene Hybrid Capture II HPV DNA testing. Am J Clin Pathol. 2008;130:765-70.
- [CrossRef] [PubMed] [Google Scholar]
- Reproducible, high-dimensional imaging in archival human tissue by multiplexed ion beam imaging by time-of-flight (MIBI-TOF) Lab Invest 2022
- [CrossRef] [Google Scholar]
- MicroRNA-based fingerprinting of cervical lesions and cancer. J Clin Med. 2020;9:3668.
- [CrossRef] [PubMed] [Google Scholar]
- MicroRNA stability in FFPE tissue samples: Dependence on GC content. PLoS One. 2016;11:e0163125.
- [CrossRef] [PubMed] [Google Scholar]
- Co-staining of microRNAs and their target proteins by miRNA in situ hybridization and immunohistofluorescence on prostate cancer tissue microarrays. Lab Invest. 2019;99:1527-34.
- [CrossRef] [PubMed] [Google Scholar]
- Analysis of microRNA niches: Techniques to measure extracellular microRNA and intracellular microRNA in situ. Methods Mol Biol. 2013;1024:157-72.
- [CrossRef] [PubMed] [Google Scholar]
- A novel approach for microRNA in situ hybridization using locked nucleic acid probes. Sci Rep. 2021;11:4504.
- [CrossRef] [PubMed] [Google Scholar]
- miRNA in situ Hybridization. BioGenex. Available from: https://biogenex.com/products/mirna-ish/?v=7516fd43adaa [Last accessed on 2022 Apr 26]
- [Google Scholar]
- MicroRNAs as markers of progression in cervical cancer: A systematic review. BMC Cancer. 2018;18:696.
- [CrossRef] [PubMed] [Google Scholar]
- Cervical cancer, papillomavirus, and miRNA dysfunction. Front Mol Biosci. 2021;8:758337.
- [CrossRef] [PubMed] [Google Scholar]
- miRNATissueAtlas2: An update to the human miRNA tissue atlas. Nucleic Acids Res. 2022;50:D211-21.
- [CrossRef] [PubMed] [Google Scholar]
- Distribution of miRNA expression across human tissues. Nucleic Acids Res. 2016;44:3865-77.
- [CrossRef] [PubMed] [Google Scholar]
- DIANA-miTED: A microRNA tissue expression database. Nucleic Acids Res. 2022;50:D1055-61.
- [CrossRef] [PubMed] [Google Scholar]




