


Translate this page into:
Stratified mucin-producing intraepithelial lesion of the cervix: A diagnostic challenge
*Corresponding author
-
Received: ,
Accepted: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
The diagnosis of glandular abnormalities of the uterine cervix by papanicolaou (Pap) test can present a variety of challenges resulting in lower test sensitivity, which include morphologic heterogeneity of glandular lesions, less efficient sampling of the endocervical zone, less obvious features of cytologic atypia and lower frequency of glandular compared with squamous lesions resulting in less observer familiarity. Several studies have noted increasing rates of adenocarcinoma of the cervix, particularly among women under the age of 40.[1] Hence, reliable identification and correct classification remain important goals in the daily practice of the cytopathologist. Although, the 2001 Bethesda system contains a separate diagnostic category for endocervical adenocarcinoma in situ,[2] there has been little emphasis on lesions with variant morphology, which are often classified within the realm of “atypical glandular cells”. Neoplasms of the cervix with morphologic overlap between squamous and glandular differentiation have long been recognized, but few studies focused specifically on these lesions and variable criteria for their classification were applied.[34] Thirteen years ago Park et al.,[5] coined the unifying term stratified mucin-producing intraepithelial lesion (SMILE) for a group of noninvasive neoplastic proliferations characterized by immature stratified cells, architecturally resembling squamous differentiation, with the added feature of cytoplasmic mucin. Until recently, there were no reports on the cytologic findings in patients presenting with SMILE.
We retrospectively examined the Pap test cytology (ThinPrep; Hologic Corporation, Marlborough, MA) of a case with the histopathologic diagnosis of SMILE. The Pap test was performed for a 51-year-old woman who had undergone loop-electrosurgical excision procedure (LEEP) at another institution and was referred to our center for specialized oncological care. Review of the LEEP specimen at the request of the attending gynecologist showed adenocarcinoma in situ of the cervix in agreement with the diagnosis rendered at the peripheral hospital. In addition, the morphologic characteristics of SMILE including immature stratified epithelium, mucin production or abundant cytoplasm, and absence of gland formation as described by Park et al.,[5] were identified [Figures 1 and 2]. The Pap test performed 1 month after the LEEP was signed out by the cytopathologist at our institution as “atypical glandular cells”. A repeat LEEP performed at our center was negative for intraepithelial lesion and malignancy. Five months later, the patient decided to undergo hysterectomy. Pathologic examination of the uterus showed residual adenocarcinoma in situ of the cervix indicating that the previous two procedures had not succeeded in eradicating the disease.
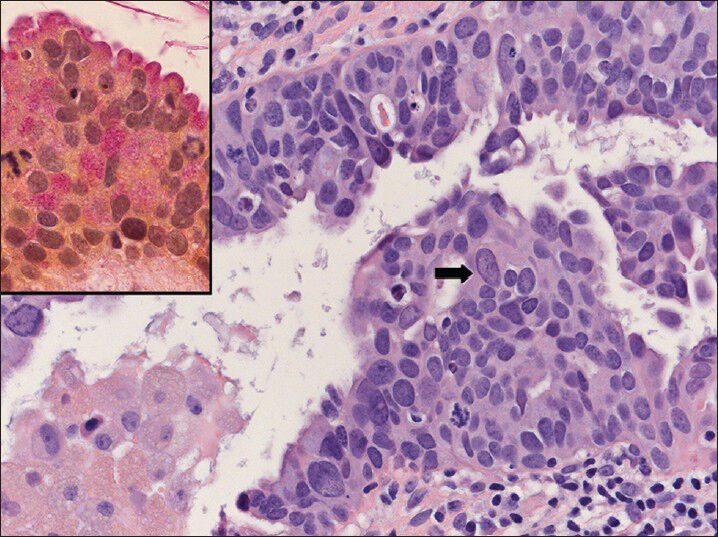
- Histology of the stratified mucin-producing intraepithelial lesion. Nuclear size variation (arrow) and cytoplasmic mucin content (inset: Mucicarmine stain) are conspicuous features. (H and E, ×40)
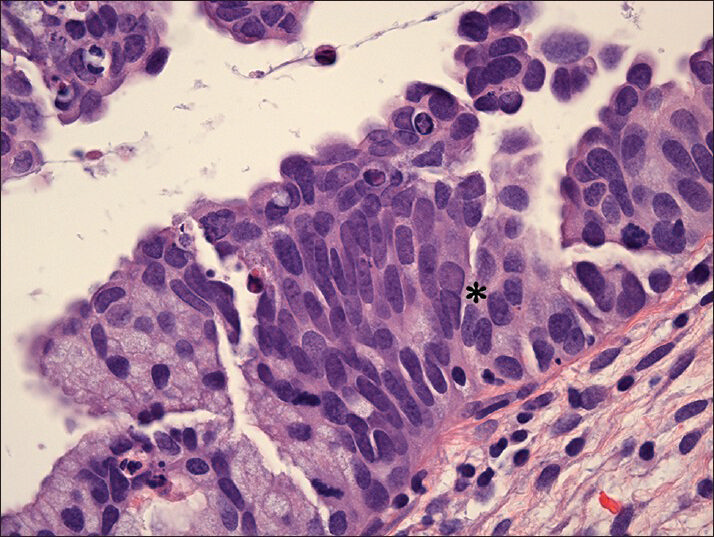
- Histology of the stratified mucin-producing intraepithelial lesion. Note the cellular crowding, presence of small nucleoli and occasional binucleation (asterisk). (H and E, ×63)
Review of the cytology revealed a hypocellular specimen with reactive changes and several cell groups that had subtle abnormalities, which corresponded well to the histopathological findings of the LEEP. These abnormalities included: (1) crowding with haphazard cell distribution (variable distances between nuclei and nuclear overlap), (2) moderate amounts of “fluffy” cytoplasm with soft margins, (3) round to ovoid nuclei with hyperchromasia and inconspicuous nucleoli, and (4) marked nuclear size variation [Figure 3]. No feathering and no rosettes or palisading strips of atypical glandular cells, architectural features generally associated with conventional adenocarcinoma in situ, were noted. The atypical cell groups were infrequent, possibly indicating that most of the lesion was inaccessible to the sampling device.
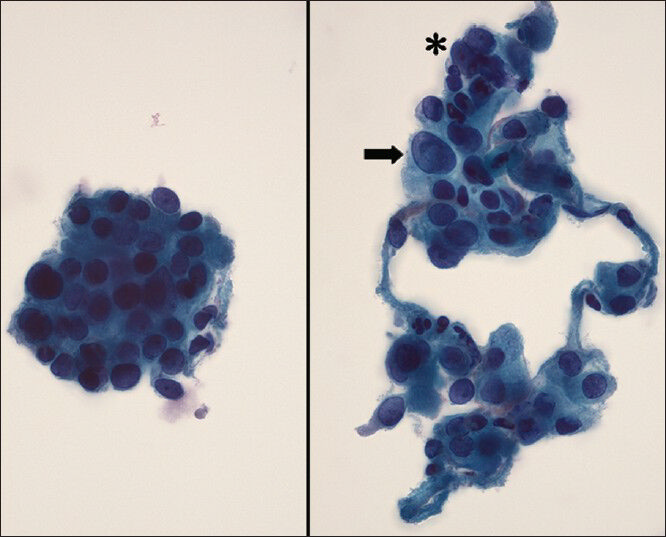
- Epithelial fragments with marked cellular crowding (left image), hyperchromasia, nuclear size variation (right image: Arrow) and occasional binucleation (right image: Asterisk) are identifiable cytologic features in this case. (Papanicolaou, ×63)
The cytologic features of SMILE have recently been described based on a case reported by Goyal and Yang[6] who also point out the subtlety of the cytologic features including mild crowding, slight hyperchromasia, indistinct nucleoli and smooth cluster edges, which may cause confusion with reactive endocervical cells and tubular metaplasia.[6] We here add another case with similar cytologic characteristics. Our case also illustrates some of the difficulties associated with the clinical management of endocervical lesions. Increasing awareness and future research including a larger number of cases showing hybrid features of squamous and glandular differentiation will need to address issues related to the optimal clinical management,[7] a question which may become more pressing considering the changing landscape of cervical cancer screening.
COMPETING INTERESTS STATEMENT BY ALL AUTHORS
The authors declare that they have no competing interests.
AUTHORS STATEMENT BY ALL AUTHORS
All authors of this article declare that we qualify for authorship as defined by ICMJE http://www.icmje.org/#author. Each author has participated sufficiently in the work and takes public responsibility for appropriate portions of the content of this article. Each author acknowledges that this final version was read and approved.
ETHICS STATEMENT BY ALL AUTHORS
As this is case report without patient identifiers, our institution does not require approval from Research Ethics Board (IRB).
EDITORIAL/PEER-REVIEW STATEMENT
To ensure the integrity and highest quality of CytoJournal publications, the review process of this manuscript was conducted under a double-blind model.(authors are blinded for reviewers and vice versa) through automatic online system.
REFERENCES
- Carcinoma and other tumors of the cervix. In: Kurman R, Ellenson L, Ronnett B, eds. Blaustein's Pathology of the Femal Genital Tract (6th ed). New York, NY, USA: Springer Science + Business Media, LLC; 2011. p. :254-303.
- [Google Scholar]
- Epithelial abnormalities: Glandular. In: Solomon D, Nayar R, eds. The Bethesda System for Reporting Cervical Cytology (2nd ed). New York,NY, USA: Springer Science + Business Media, LLC; 2004. p. :123-56.
- [Google Scholar]
- Histopathologic classification of cervical carcinomas and recognition of mucin-secreting squamous carcinomas. Int J Gynecol Pathol. 1993;12:64-9.
- [Google Scholar]
- Mucin production in cervical intraepithelial neoplasia and in stage 1b carcinoma of cervix with pelvic lymph node metastases. Br J Obstet Gynaecol. 1987;94:467-72.
- [Google Scholar]
- Stratified mucin-producing intraepithelial lesions of the cervix: Adenosquamous or columnar cell neoplasia? Am J Surg Pathol. 2000;24:1414-9.
- [Google Scholar]
- Cytologic features of stratified mucin producing intraepithelial lesion of the cervix-A case report. Diagn Cytopathol 2013 [Epub ahead of print]
- [Google Scholar]
- Follow-up of patients with SMILE (stratified mucin producing intraepithelial lesion) on the cervix-A dilemma. Eur J Obstet Gynecol Reprod Biol. 2010;148:207-9.
- [Google Scholar]




