


Translate this page into:
Amylase crystalloids in fine needle aspiration cytology of parotid gland: A diagnostic challenge
*Corresponding author
-
Received: ,
Accepted: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
Several types of crystalloids may be seen in fine needle aspiration cytology of benign or malignant lesions of the salivary gland.[12] Due to their rarity, they may lead to confusion in diagnosis. Amylase type crystalloids (sometimes named nontyrosine crystals) are rarely found angular, nonbirefringent rectangular formed structures, with geometric shapes ranging between 5 μ and 500 μ in size and stained orange with Papanicolaou (PAP), dark blue with Diff-Quik® (DQ) and pink with Hematoxylin-Eosin (HE) stain.
They were first defined in salivary gland cysts in 1983 by Takeda and Ishikawa.[13] Amylase crystalloids may also be observed in cystic sialadenitis as much as in cystic lesions.[1] We have presented here a case with cystic and chronic sialadenitis in the parotid gland, containing amylase crystalloids.
The ultrasonographic assessment performed on a 58-year-old female patient who had applied with a complaint of swelling in the frontal part of the left ear and on the left part of the neck resulted in the detection of a lesion at a size of 12.5 mm × 11 mm in the lower zone of the left parotid [Figure 1] and lymph node at a diameter of 1 cm in the left cervical area.

- Ultrasonographic picture of the parotid mass
Ultrasound-guided fine needle aspiration was performed by cytopathologist (N.P) with the preliminary diagnosis of the parotid tumor. About 0.2 cc of a mucoid fluid at an off-white color was aspirated. The slides were stained with DQ, PAP and HE.
Cytologic findings showed mixed-type inflammatory elements, proliferated salivary gland acinar cells, reactive atypical salivary gland ductal cells as well as square, cuboid, needle, rectangular, rhomboid or bar-shaped crystalloids [Figure 2a–d]. The crystalloids were stained bright orange with PAP; deep blue with DQ and eosinophilic with HE [Figure 3a and b]. Birefringence of the crystalloids was not observed by polarized light. The case was reported as cystic and chronic sialadenitis containing amylase crystalloids. The patient was monitored, and no growth was detected in the 2 years follow-up.
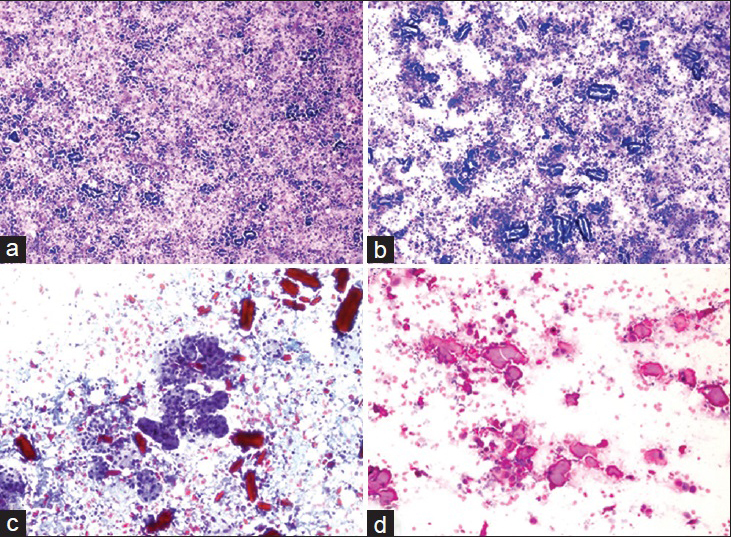
- Various cytologic images of the amylase crystalloids on different power and stains. (a) Diff-Quik®, ×100. (b) Diff-Quik®, ×200. (c) Papanicolaou, ×200. (d) H and E, ×400
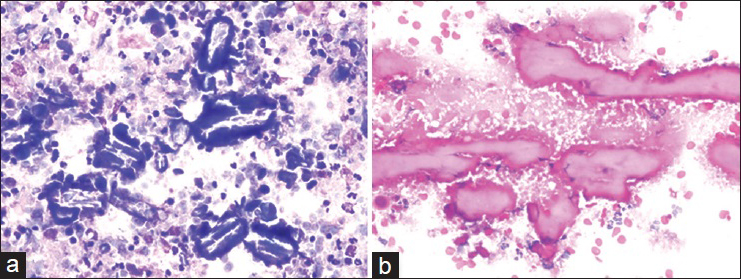
- Images of crystalloids at high power magnification with representative morphology. (a) Diff-Quik®, ×400. (b) H and E, ×400
Many crystals such as amylase, tyrosine, collagenous crystalloids, oxalate and intraluminal crystals may be observed in the fine needle aspiration smears of salivary gland lesions.[124]
It is important to differentiate amylase crystalloids, which are geometric-shaped structures larger than 5 μm microscopically, from other crystalloids. Because, although crystalloids may be seen in malignant salivary gland tumors, amylase crystalloids accompany benign lesions.[15]
The different types of crystals/crystalloids in relation to benign and malignant lesions and special stains/methods of detection are outlined below.
Intraluminal crystalloids show a structure with geometrical shapes like amylase crystalloids. However, intraluminal crystalloids are dense, amorphous, filled with eosinophilic substance and at a size of 100 μ. Intraluminal crystalloid are reported to be seen in malignant salivary gland tumors.[6]
Amylase crystalloids have more translucent appearance and are generally at a size of 500 μ. They are stained orange with PAP, dark blue with DQ® and pink with HE. Both intraluminal and amylase crstalloids are nonbirefringent.
Amylase crystalloids are so far encountered with only in benign lesions including chronic sialadenitis, unilocular cysts, lymphoepithelial cysts and Warthin's tumor.[17]
Collagenous crystalloids are seen as radial and fusiform fibers of eosinophilic collagen on HE stain. These crystalloids stain bright blue on trichrome stain, indicating the presence of Type I collagen and are also positive on Snook Reticulin Stain, indicating the presence of Type III collagen. They are birefringent. Collagenous crystalloids are reported to be seen in pleomorphic adenomas, myoepitheliomas and also myoepithelial carcinomas.[56]
Tyrosine crystals appear in an eosinophilic, refractile, flower-like shape with blunt ends (petal shaped) on HE stain. Tyrosine crystalloids are reactive with Millon reagent and are positive with diazotization-coupling reaction. They are nonbirefringent. Tyrosine crystals are mainly identified in pleomorphic adenomas and also rarely encountered in malignant salivary gland neoplasms such as carcinoma ex pleomorphic adenoma, adenoid cystic carcinoma, low-grade adenocarcinoma.[1256]
In conclusion, amylase crystalloids are not substances that may appear very frequently in parotid fine needle aspiration. They may accompany especially nonmalignant benign, chronic inflammatory lesions. They are rarely observed.
We wanted to present our case in the light of literature for the purpose of highlighting the fact that crystalloids may lead to diagnostic challenges in parotid fine needle aspiration. We also focused on the representative cytomorphology of the crystalloids.
COMPETING INTERESTS STATEMENT BY ALL AUTHORS
The authors declare that they have no competing interests.
AUTHORSHIP STATEMENT BY ALL AUTHORS
Each author has participated sufficiently in the work and takes public responsibility for appropriate portions of the content of this article. Each author acknowledges that this final version was read and approved.
ETHICS STATEMENT BY ALL AUTHORS
This manuscript is a case description in form of a letter. Therefore, institutional ethical approval is not mandatory.
LIST OF ABBREVIATIONS
PAP = Papanicolaou
HE = Hematoxylin-Eosin
EDITORIAL/PEER-REVIEW STATEMENT
To ensure the integrity and highest quality of CytoJournal publications, the review process of this manuscript was conducted under a double-blind model (authors are blinded for reviewers and vice versa) through the automatic online system.
ACKNOWLEGMENT
Presented in part in form of a poster at the 24th National Pathology Congress in Trabzon. Turkey in 19-23 November 2014.
REFERENCES
- Amylase crystalloids on fine-needle aspiration of salivary gland. Turk Patoloji Derg. 2010;26:153-5.
- [Google Scholar]
- A-amylase crystalloid granuloma in the parotid gland. Diagn Cytopathol. 2015;43:114-6.
- [Google Scholar]
- Crystalloids in salivary duct cysts of the human parotid gland. Scanning electron microscopical study with electron probe X-ray microanalysis. Virchows Arch A Pathol Anat Histopathol. 1983;399:41-8.
- [Google Scholar]
- Sialadenitis with crystalloid formation. Fine needle aspiration cytodiagnosis of 15 cases. Acta Cytol. 2003;47:1-4.
- [Google Scholar]
- Collagenous crystalloids in myoepithelial carcinoma: Report of a case and review of the literature. Am J Clin Pathol. 2008;130:355-62.
- [Google Scholar]
- Intraluminal crystalloids in malignant salivary gland tumors (electron microscopic and X-ray microanalytic studies) J Laryngol Otol. 1987;101:1175-81.
- [Google Scholar]




