


Translate this page into:
Evaluation of a triple combination of cytokeratin 20, p53 and CD44 for improving detection of urothelial carcinoma in urine cytology specimens
*Corresponding author
-
Received: ,
Accepted: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
Atypical urine cytology results trigger cystoscopy or molecular tests, both of which are costly, complex and difficult to perform tests. Several immunostains are being investigated to improve cancer detection; however, cytology material is limited and restricts the use of multiple immunostains. This study was designed to determine the utility of a cocktail of three stains, cytokeratin (CK20), p53 and CD44 in urine cytology samples for improving the detection of urothelial carcinoma.
Materials and Methods:
Urine cytology specimens with cell blocks containing adequate cytologic material between 2005 and 2010 and subsequent follow-up biopsy and/or Urovysion test (102 cases including 29 negative, 56 atypical and 17 malignant) were included in the study and evaluated with the triple stain. Results were first validated on the positive and negative cases and then applied to the atypical cases to determine the utility in the diagnosis of urothelial carcinoma.
Results:
Based on the validation and published literature, two distinct immunoprofiles were defined – malignant, characterized by at least five CK20 and/or p53 positive atypical cells and reactive, all other staining patterns. The malignant immunoprofile showed 88% sensitivity, 78% specificity, 74% positive predictive value (PPV) and 90% negative predictive value (NPV) for detecting urothelial carcinoma. These values improved to 95% sensitivity and 96% NPV when low-grade urothelial carcinoma cases were excluded.
Summary:
Our results indicate that the triple stain is an inexpensive, easy to perform test most useful for differentiating high-grade urothelial carcinoma from its mimics. However Inclusion of CD44 in the cocktail did not provide additional value and is best excluded.
Keywords
Carcinoma cytokeratin 20
cytology
p53
urine

INTRODUCTION
Bladder cancer is the fourth most common cancer among American men. It is estimated that 73,510 new cases of bladder cancer will be diagnosed in 2012 with over 14,880 deaths.[1] More than 90% of bladder cancers are urothelial carcinomas and almost 80% of these are superficial, non-muscle-invasive tumors.[2] Despite their favorable prognosis a significant proportion (37-54%) of these tumors recur and up to 15% progress to a higher stage[3] necessitating lifelong follow-up and surveillance.
The detection and surveillance of urothelial carcinoma relies primarily on cystoscopy, cytological examination of urine specimens and increasingly various molecular and genetic tests including the Urovysion® Test (Abbott Laboratories. Abbott Park, Illinois, USA). Urine cytology, the most commonly used noninvasive test, is very efficient in the detection of primary and recurrent high-grade urothelial carcinoma and carcinoma in situ with sensitivity and specificity of up to 98%.[4] It is, however, severely restricted in its capability of detecting low-grade urothelial carcinoma with sensitivity and specificity of 8.5% and 50% respectively.[56] In addition, the cytologic diagnosis of urothelial carcinoma is frequently challenged by atypia seen in association with benign conditions such as inflammation, lithiasis, viral cytopathic changes and therapy induced changes. The significant morphologic overlap among these categories frequently results in an atypical or indeterminate cytologic diagnosis causing uncertainty regarding subsequent management.[7] Atypical cytologic diagnoses constitute a significant proportion of all urine cytology specimens with reported rates ranging from 2% to 23%.[5689] The rate at this institution is 20%. To address this problem various ancillary tests such as the multitarget multicolor fluorescent in situ hybridization (FISH) assay (Urovysion), a Food and Drug Administration approved test designed to detect aneuploidy for chromosomes 3, 7, 17 and loss of the 9p21 locus for detection and surveillance of bladder cancer has been developed. Although many have reported a higher sensitivity with Urovysion for all grades and stages of urothelial carcinoma than conventional cytology, others have found it to be of limited value.[101112] Its high cost and complex laboratory procedures also limits its widespread use.[13]
Recently, immunohistochemical stains including cytokeratin 20 (CK20), CD44 (standard isoform), p53 and Ki-67 (MIB1 antibody) have been examined by several studies singly and in various combinations for their utility in identifying malignant urothelial lesions.[141516] Although studies using single stains have reported improved detection rates, the addition of multiple stains has been shown to mitigate the high false positive results from staining of benign entities.[71517181920212223]
Based on these findings, this study was designed to determine the utility of a triple cocktail of CK20, p53 and CD44 on urine cytology samples for the diagnosis of urothelial carcinoma and differentiating it from benign mimics. Cytology specimens frequently have limited material for testing which makes a triple immunohistochemical stain appealing. The combination of CK20, CD44 and p53 as a triple cocktail on urine cytology specimens has yet to be reported to our knowledge. As an ancillary test, it has the potential for providing a simple, cost-effective modality for urine cytology specimens with an atypical diagnosis.
MATERIALS AND METHODS
A search of our intradepartmental database revealed a total of 8401 cases of urine cytology between 2005 and 2010 of which 799 had cell blocks. 125 cases with diagnostic material on the cell blocks were randomly selected from each of the cytologic categories of negative, positive and atypical. Urine specimen categories included voided (54 cases), bladder washings (36 cases), kidney washings (22 cases), site unspecified (10 cases), catheterized (2 cases) and ureteral washings (1 case) period. Follow-up information in the form of biopsy or resection and/or results of Urovysion testing performed concurrently or within 7 months of diagnosis was available in 102 (81.6%) cases. These cases comprised the study group. Urovysion testing of urine samples is performed in our laboratory in accordance with the manufacturer's recommendations and on the request of treating physicians.
Cell blocks were prepared on all urine specimens with the sufficient sediment following centrifugation at 1866 rpm for 10 min. The cell pellet was dislodged from the bottom of the tube, packaged in tissue paper, placed in a cassette, fixed in 10% formalin and processed per standard protocols for paraffin embedding and staining with hematoxylin and eosin. One additional 4 μm slide was prepared from each cell block for immunostaining.
Immunostaining
p53 (Cell Marque, Rocklin, CA clone DO7), CD44 standard isoform (Dako, Carpinteria, CA, clone MRQ-13) and CK20 (Ventana, Tucson, AZ, clone Ks20.8) were applied as a triple stain cocktail on 4 μm thick sections from the cell block of each case in the study group. Immunostaining was performed using the Ventana Benchmark XT. A dual staining protocol was followed per the manufacturer's instructions. Antigen retrieval was performed with citrate buffer (pH 6.0) on a Dako PT-Link module. Prediluted p53 as provided by the manufacturer and CD 44 (1:50) were applied first and stained with Ventana ultraview DAB kit to achieve brown staining. This was followed by prediluted CK20 as provided by the manufacturer which was stained with Ventana ultraview Red Kit to produce red staining. Positive controls included urothelial carcinoma for CK20, lymph node tissue for p53 and tonsillar tissue for CD44.
Positive staining for CK20 was visualized as red cytoplasmic stain, for CD44 as a brown membranous stain and for p53 as brown nuclear stain. Immunostained slides were reviewed by two Cytopathologists.
The study was performed in two parts
Firstly, the triple stain was validated on known negative and positive urine samples with cell blocks with the aim of testing its performance on cytology specimens. The respective cytologic diagnoses were confirmed by review of smears and follow-up biopsy material.
Secondly, the triple stain was evaluated on the cell blocks of cases with atypical cytology diagnosis by two Cytopathologists blinded to the results of subsequent follow-up and/or biopsy with the aim of determining its efficacy in detecting cancer. Results of the triple stain were then correlated with follow-up diagnoses in order to determine its utility in the diagnosis and triage of patients.
RESULTS
Included in the 102 cases with follow-up information were 29 cases with a cytology diagnosis of negative for malignant cells, 56 cases with a cytology diagnosis of atypical cells and 17 cases with a cytology diagnosis of positive for malignant cells.
The 21 cases had biopsy/resection and the Urovysion test, 54 cases had biopsy/resection only (concurrent to 106 days, mean = 16.4 days) and 27 cases had the Urovysion test only (concurrent to 134 days, mean = 12.2 days).
The 21 cases with both biopsy/resection and Urovysion on the follow-up included eight cases with Urovysion performed at the time of biopsy/resection, seven cases with Urovysion performed 45-215 days after biopsy/resection (mean 114.7 days), two cases with Urovysion performed at day 61 and day 102 after biopsy/resection, respectively and four cases with biopsy/resection following the urine cytology 10 days to 153 days (mean = 55.8 days) later and Urovysion testing 38 days to 207 days (mean = 112.3 days) later.
A total of 42 carcinomas were detected on follow-up. These included 37 high-grade urothelial carcinomas and five low-grade urothelial carcinomas. One case was positive with the Urovysion test only, showing aneuploidy consistent with urothelial carcinoma. No follow-up biopsy was available. This case was regarded as a carcinoma for purposes of this study as was a second case with an abnormal Urovysion test at five months that developed carcinoma at 13.5 months.
Validation
The 29 cases with negative cytology diagnosis and the 17 cases with positive cytology diagnosis were used for the validation. All 29 cases with negative cytology were negative on follow-up biopsy/resection at 7 months. One case showed an abnormal Urovysion test at five months, followed by a positive cytology at approximately 8 months and eventually showed high-grade urothelial carcinoma on biopsy 13.5 months after the negative cytology. Of the 17 positive urine samples, 14 were diagnosed as high-grade on cytology, 1 as low-grade and 2 as not otherwise specified. The diagnosis was confirmed on all cases on follow-up biopsy/resection with the exception of one case of high-grade urothelial carcinoma on cytology in which the only information available was a positive Urovysion test. The two cases diagnosed as not otherwise specified were high-grade on follow-up biopsy/resection.
The three components of triple stain were evaluated individually and in combination on the cell blocks of the negative and positive cases.
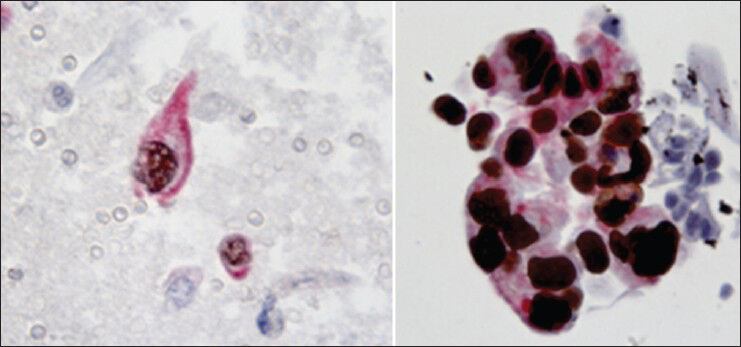
Positive staining was noted in normal cells in variable amounts. CK20 positivity was most frequently observed in the cytoplasm of normal superficial cells identified as medium to large sized urothelial cells with rounded luminal surfaces, scalloped borders, abundant cytoplasm and often multiple nuclei. The presence of abundant cytoplasm in cells with low nuclear to cytoplasm ratio was considered as the hallmark of superficial cells [Figure 1]. p53 positivity was noted rarely in superficial cells in occasional cases while CD44 positivity was seen in some cases in basal cells identified as small cells with small round bland nuclei and scant to moderate cytoplasm. An effort was made to exclude normal cells from the interpretation of the triple stain. Results of the staining pattern noted only in morphologically atypical urothelial cells were recorded. Atypical morphology was defined as urothelial cells displaying increased nuclear to cytoplasmic ratios, nuclear hyperchromasia, coarse chromatin and/or irregular nuclear contours. Results are summarized in Table 1.
- Superficial urothelial cells highlighted by cytokeratin20 immunostain (×600)

The combination of CK20 and/or p53 positivity yielded the most discriminating results for differentiating benign and malignant cells. Thus, based on our initial findings [Table 1] and on those published in literature we chose to categorize the results of the triple stain as:
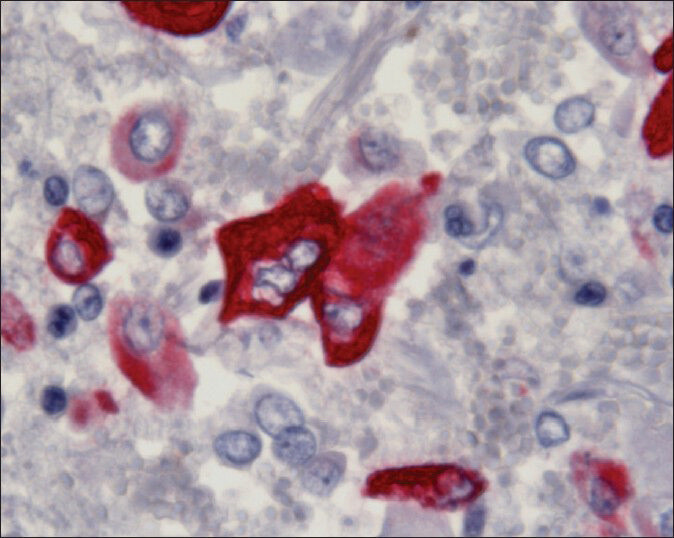
1. A malignant immunoprofile: This was defined as the presence of at least five morphologically atypical cells staining for CK20 (cytoplasmic red) and/or p53 (nuclear brown) [Figure 2]. The cut-off of five cells was arbitrarily defined.
- Examples of atypical cells expressing a malignant immunoprofile. Atypical cells are positive for p53 (brown nuclear stain) and cytokeratin20 (red cytoplasmic stain) immunostains (×600)
2. A reactive immunoprofile: This was defined as positive staining for CD44 in the absence of CK20 and/or p53 positivity. For simplicity any case with (a) fewer than five atypical urothelial cells exhibiting CK20 positivity and/or p53 positivity in the absence of CD44 positivity or (b) negative staining for all three components of the triple stain was included in this category [Figure 3].
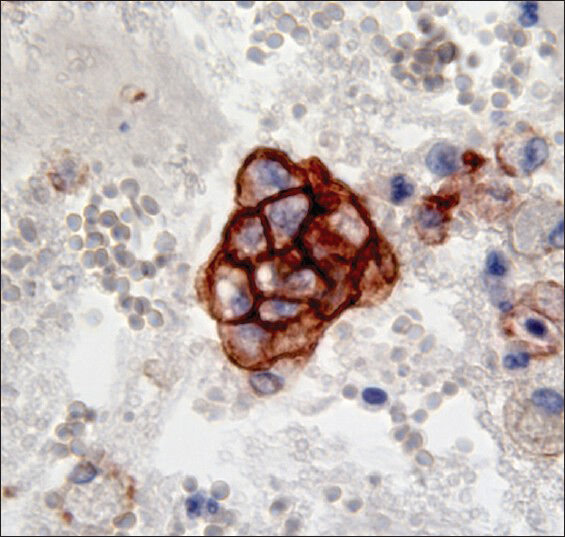
- Cluster of basal cells expressing a benign/reactive immunoprofile of membranous positivity for CD44 (brown cytoplasmic stain) with negativity for p53 and Cytokeratin (×600)
Results of triple stain in negative cytology
Three (10%) of the 29 negative cases demonstrated a malignant immunoprofile, each with a distinct pattern; CK20+p53+CD44+ in one case, CK20+CD44+p53− in one case and CK20+p53−CD44− in one case [Table 1]. Two of these samples were obtained from patients with previous diagnoses of high-grade urothelial carcinoma and included the case with the abnormal FISH five months later and subsequently high-grade urothelial carcinoma. The other case had a negative follow-up. The third case was a bladder urine sample obtained at the time of a transurethral resection for benign prostatic hyperplasia. Urothelial cells were present singly and in clusters and showed reactive atypia. No malignancy was identified in the concurrent bladder neck biopsy.
Results of triple stain in positive cytology
Positivity for all three components of the triple stain (CK20+p53+CD44+) was seen in 7/16 (44%) cases. p53 positivity was observed with variable CK20 and CD44 positivity. Positivity for all three of the stains was not observed within the same atypical cell in any cases. Seven cases were CK20+/p53+/CD44−, six of which showed p53 and CK20 positivity within the same atypical cells. One case showed CK20+/p53−/CD44− and one showed CK20−/p53+/CD44+ with atypical cells demonstrating mostly p53 positivity with occasional cells showing both p53 and CD44 positivity [Table 1].
A positive triple stain was associated with a subsequent diagnosis of urothelial carcinoma with a sensitivity of 94%, specificity of 93%, a of 90% and a of 96%. One carcinoma case that was falsely negative was low-grade urothelial carcinoma [Table 2].

Performance of the triple stain in atypical cytology
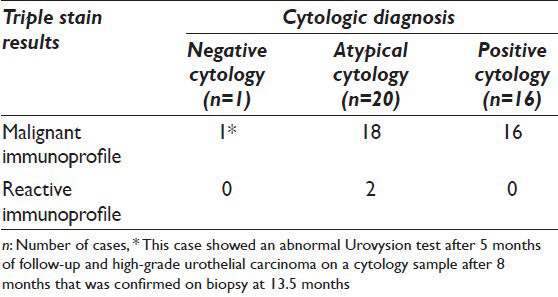
Figure 4 summarizes results of the triple stain on atypical cytology specimens. The 25 cases with a reactive immunoprofile were all CK20 and p53 negative; CD44 was positive in only a minority (7/25, 29%). 21 of these 25 cases had negative follow-up. The remaining four cases showed urothelial carcinoma on follow-up-two low-grade urothelial carcinomas and two high-grade urothelial carcinomas.

- Results of the triple stain on urine cytology specimens diagnosed as atypical. Of the four false negative cases two were low-grade urothelial carcinomas and two were high-grade urothelial carcinomas, one of which was confirmed on biopsy. The second case had an abnormal Urovysion test with a negative biopsy. Of the 20 true positive cases 17 were high-grade urothelial carcinomas, two were low-grade urothelial carcinomas and one case had an abnormal Urovysion test with no follow-up biopsy
The remaining 31 of the 56 cases with atypical cytology had a malignant immunoprofile; CK20+p53+CD44+in eight cases, CK20+p53+CD44−in nine cases, CK20+p53−CD44+in one case, CK20+p53−CD44−in nine cases, CK20 − p53 + CD44 + in two cases and CK20 − p53+CD44− in two cases. Carcinoma was present in 19 (61%) of these cases on follow-up excisions, two of which were low-grade urothelial carcinoma on biopsy. One case showed an abnormal Urovysion test result on follow-up. Biopsy information was not available in this case. The remaining 11 (36%) cases were negative on follow-up.
Overall 21/25 cases with atypical cytology and a reactive triple stain immunoprofile were associated with a negative follow-up. 20/31 cases with atypical cytology and a malignant triple stain profile were associated with malignancy at follow-up. Four carcinomas were missed of which two were low-grade urothelial carcinoma. The triple stain demonstrated false positivity in 11/56 (20%) cases. Sensitivity and specificity of the triple stain for atypical cytology specimens was 83% and 66% respectively with a PPV of 65% and NPV of 84%. The sensitivity and NPV improved to 90% and 91% respectively when low-grade urothelial carcinoma cases were excluded.
The 21 cases within our study group had Urovysion testing and biopsy/resection. A comparison of the Urovysion results and triple stain results among these cases is summarized in Table 3. Both tests yielded similar results.

Within the entire study group of 102 cases there were five cases of biopsy proven low-grade urothelial carcinoma, only one of which was diagnosed on cytology. Both the Urovysion test and the triple stain were negative in this case. The remaining four cases of low-grade urothelial carcinoma had cytologic diagnoses of atypical cells. Two of these cases showed a malignant immunoprofile (CK20+/p53+/CD44+ and CK20+/p53−/CD44−). The remaining two cases demonstrated the reactive immunoprofile. Urovysion performed on one of these cases with the reactive immunoprofile was also normal.
The cohort included urine samples from a total of 37 high-grade urothelial carcinomas, 35 of which demonstrated the malignant immunoprofile [Table 4]. Two cases were falsely negative and demonstrated the reactive immunoprofile. Both of these cases contained atypical cells in the urine sample. One of these was diagnosed as high-grade urothelial carcinoma on a biopsy performed two weeks later. The second case showed an abnormal Urovysion test. The concurrent biopsy was negative.
To summarize, the triple stain correctly identified 37 of the 42 cases (88%) that proved to be malignant on follow-up. It failed to identify five of the urothelial carcinomas, three of which were low-grade. 13 cases stained falsely positive (a positive triple stain with negative follow-up), rendering an overall sensitivity of 88%, a specificity of 78%, a PPV 74% and a NPV of 90% [Table 2]. These values improved considerably when low-grade urothelial carcinoma cases were excluded with sensitivity rising from 88% to 95% and NPV increasing from 90% to 96% [Table 2].
DISCUSSION
This study demonstrates that the triple stain, a cocktail of CK20, p53 and CD44 is easily performed on cell block samples of urine cytology and demonstrates sensitivity and specificity of 88.1% and 78.3% respectively for detecting urothelial carcinoma. It is more effective in detecting high-grade urothelial carcinoma with a sensitivity of 94.6% and specificity of 78.3%. Low-grade urothelial carcinomas demonstrate a high false negative rate. The triple stain may thus be applied to atypical cytology samples for distinguishing urothelial carcinoma from its mimics. In addition, the higher test sensitivity and NPVs in atypical samples than specificity and PPVs suggests that the triple stain may be effectively used as a triage for selecting samples for further testing.
Of the three markers CK20 and p53 proved to be useful in identifying cases with subsequent carcinoma. CD44 was not very reliable being present only in a minority of cases and is best excluded from the cocktail.
A large number of adjunctive markers are being investigated to improve the detection of urothelial carcinoma. Several urine based and cell based markers are available.[24] Of these p53 and CK20 used in conjunction with CD44 are emerging as useful indicators of neoplastic change and prognosis in urothelial proliferations. These have primarily been investigated in surgical specimens for improving diagnostic accuracy of carcinoma.[716172526] We report the results of using these stains as a triple cocktail on cell blocks prepared from cytology samples to determine their efficacy as a tool for improving the detection of urothelial carcinoma.
CK20 is a marker of cellular differentiation and is considered a useful and reliable marker of neoplastic change in urothelial cells.[182527282930] In normal urothelium CK20 expression is confined to umbrella cells and occasional intermediate cells.[2527] This pattern is lost in abnormal urothelium where CK20 is seen in deeper or in all cell layers.[25] Negative staining or positive staining in only the superficial umbrella cell layer or in the upper one third of the urothelium is reported in 92% of benign/reactive urothelium.[19] Diffuse full thickness staining is present in 22-90% of cases of urothelial carcinomas, with invasive carcinomas being less frequently positive as compared to carcinoma in situ.[71731323334] Cytokeratin 20 immunoexpression has been found to be non-discriminatory in 11-28% of cases of carcinoma in situ due to lack of CK20 expression.[7173132]
Previous studies have demonstrated that CK20 immunocytology in voided urine samples exhibit greater sensitivity and reliability than standard cytology in the diagnosis of urothelial carcinoma. Thus, CK20 may provide a useful tool for triaging atypical cases into high and low risk categories and may be helpful in confirming malignancy when morphology alone is inadequate.[1520] Melissourgos et al., reported an increase in sensitivity from 54% to 65% and an increase in specificity from 86% to 91% when using CK20 over cytology alone for the detection of malignancy.[35] Others have reported sensitivities of 70-77% and specificities of 83% to 91%.[1421] Our data is comparable and shows CK20 positivity in 33/42 cases (79%) of carcinoma and negativity in 9/42 cases (21%) [Table 1] yielding specificity of 80%.
P53 is a tumor suppressor gene involved in transcriptional regulation. Nuclear overexpression by immunohistochemistry has been shown to correlate with p53 mutations, which are a common event in urothelial carcinomas. Overexpression is reported in 40% to 80% of urothelial carcinomas, more commonly in high-grade lesions and is considered a marker of disease progression.[71736373839] Strong diffuse positivity in >50% of cells is characteristic of neoplastic epithelium, while in nonneoplastic and reactive urothelium, expression of p53 is noted to vary from negative to weak, patchy, positivity in basal and parabasal intermediate cells.[71740] The sensitivity and specificity of p53 for the detection of urothelial carcinoma in voided urine has been reported to range from 24% to 37%, with specificity ranging from 75% to 100%.[4142] Our results with p53 immunostaining alone show positivity in 28/42 (67%) of carcinoma cases and negativity in 14/42 (33%) [Table 1] resulting in a sensitivity of 67% and specificity of 85%. These values are concurrent with those described in the literature.
The evaluation of the immunostaining pattern on surgical specimens for both CK20 (abnormal full thickness staining vs. normal superficial staining) and p53 (abnormal diffuse strong positivity vs. normal patchy weak basal staining) is largely dependent on tissue architecture, a feature that cannot be relied on in cytology specimens. Thus, a cut-off of more than or equal to five atypical cells with positive staining was utilized with the intention of reducing the false positive cases.
CD44 is a transmembrane glycoprotein involved in cell adhesion and plays an important role in lymphocyte homing and activation, cell motility, tumor metastasis and intercellular interactions with cytoskeletal-related components including actin and ankyrin and is a receptor for hyaluronic acid.[74344] It has been shown to be a prognostic factor in urothelial carcinoma and to be increased in expression in irritated bladder mucosa.[2945464748] A report by McKenney demonstrated the usefulness of CD44 as part of a panel of three immunostains in identifying the carcinoma in situ of the bladder. They showed the absence of CD44 staining in atypical cells of biopsy specimens is supportive of neoplasm, whereas full thickness staining of the urothelium is supportive of a reactive process.[7] Alone or in combination with CK20 and p53, CD44 did not prove to be useful in detecting neoplasm within our study group. CD44 was positive in only 12/60 cases (20%) with negative or atypical cytology diagnoses, which later proved to be benign [Table 1]. In addition, it showed an inconsistent rate of positivity, from 3% to 53%, among cases of malignancy [Table 1]. CD44 is therefore redundant and is best excluded from the cocktail. Its exclusion does not change the detection rate and will reduce the cost of the test.
Detection of carcinoma was improved over cytology alone when CK20 and p53 were applied in combination. The malignant immunoprofile was noted in 31 cases with an atypical cytology diagnosis of which 20 were urothelial carcinoma on subsequent follow-up. Four carcinomas showed a reactive immunoprofile, two of which were low-grade urothelial carcinoma, one a high-grade urothelial carcinoma, while the fourth case showed an abnormal Urovysion test only, the concurrent biopsy was negative. The high false positivity suggests that this combination is best used as a triage for additional testing in atypical cases.
The overall sensitivity and specificity of the triple stain in the detection of malignancy in urine specimens was 88% and 78%, respectively with an increase in sensitivity to 95% when low-grade urothelial carcinomas were excluded from the study group [Table 2]. This suggests that, like the Urovysion test, the triple stain shows greater capability for detecting high-grade urothelial carcinomas.
The sensitivity of Urovysion for the detection of urothelial carcinoma ranges from 58% to 100% depending on the grade and stage of the tumor, with higher sensitivity for higher grade and stage tumors.[4950] Overall, it is reported to have a higher sensitivity for all grades and stages of urothelial carcinoma than conventional cytology alone.[50515253] The specificity of the Urovysion test for the detection of urothelial carcinoma ranges from 77% to 98%.[50515253] Because of the reported high sensitivity and specificity of the Urovysion test and because of its common use for surveillance, it was used as a determinant of malignancy in this study when an abnormal result was obtained in the absence of a negative biopsy. Although, it is known that the UroVysion test may display an “anticipatory effect” in cases of recurrent urothelial carcinoma, i.e., a case with negative or atypical cytology and negative cystoscopy shows a positive Urovysion test result prior to developing a recurrence.[53] Yoder et al., demonstrated that this occurs in 26% of patients under surveillance for recurrent urothelial carcinoma. Approximately, 65% of this subset develops recurrent urothelial carcinoma within 29 months.[54] In the current study, one patient with a history of urothelial carcinoma had a negative cytology specimen and a malignant triple stain profile. The Urovysion test was positive five months later followed by a recurrence of urothelial carcinoma raising the question of a similar anticipatory effect. Further larger scale studies are warranted to determine this.
SUMMARY
Our results indicate that the triple stain is a useful adjunct in confirming neoplasm in cell block preparations of urine cytology specimens and for triaging of atypical cases for additional work-up. The most appropriate setting for utilizing the triple stain is in distinguishing high-grade urothelial carcinoma from degenerative atypia or therapy effect in the setting of ongoing treatment. The triple stain is restricted in its ability to detect low-grade urothelial carcinomas. Inclusion of CD44 in the triple stain did not provide additional value and is best excluded. The utility of a combination of CK20 and p53 are needed in a prospective setting. In addition, the feasibility of the application of a cocktail of the two stains on direct smears needs to be investigated.
COMPETING INTERESTS STATEMENT BY ALL AUTHORS
The author declare that they have no competing interests.
AUTHORSHIP STATEMENT BY ALL AUTHORS
All authors of this article declare that we qualify for authorship as defined by ICMJE http://www.icmje.org/#author.
Each author has participated sufficiently in the work and takes public responsibility for appropriate portions of the content of this article.
Each author acknowledges that this final version was read and approved.
ETHICS STATEMENT BY ALL AUTHORS
This study was conducted with approval from Institutional Review Board (IRB) of the institution associated with this study.
Authors take responsibility to maintain relevant documentation in this respect.
EDITORIAL/PEER-REVIEW STATEMENT
To ensure the integrity and highest quality of CytoJournal publications, the review process of this manuscript was conducted under a double-blind model (authors are blinded for reviewers and vice versa) through automatic online system.
Available FREE in open access from: http://www.cytojournal.com/text.asp?2013/10/1/25/123784
REFERENCES
- Available from: http://www.cancer.gov/cancertopics/types/bladder
- Natural history of superficial bladder cancer. Prognostic features and long-term disease course. Urol Clin North Am. 1992;19:429-33.
- [Google Scholar]
- Prognostic parameters in superficial bladder cancer: An analysis of 315 cases. J Urol. 1982;127:250-2.
- [Google Scholar]
- Urine cytology discrepancies: Frequency, causes, and outcomes. Am J Clin Pathol. 2007;127:946-53.
- [Google Scholar]
- Accuracy of urine cytology and the significance of an atypical category. Am J Clin Pathol. 2009;132:785-93.
- [Google Scholar]
- Discriminatory immunohistochemical staining of urothelial carcinoma in situ and non-neoplastic urothelium: An analysis of cytokeratin 20, p53, and CD44 antigens. Am J Surg Pathol. 2001;25:1074-8.
- [Google Scholar]
- Malignant atypical cell in urine cytology: A diagnostic dilemma. Cytojournal. 2006;3:28.
- [Google Scholar]
- Diagnostic significance of ‘atypia’ in instrumented versus voided urine specimens. Cancer. 2008;114:270-4.
- [Google Scholar]
- UroVysion compared with cytology and quantitative cytology in the surveillance of non-muscle-invasive bladder cancer. Eur Urol. 2007;51:1275-80.
- [Google Scholar]
- Reflex UroVysion testing in suspicious urine cytology cases. Cancer. 2009;117:7-14.
- [Google Scholar]
- Comparative diagnostic value of urine cytology, UBC-ELISA, and fluorescence in situ hybridization for detection of transitional cell carcinoma of urinary bladder in routine clinical practice. Urology. 2007;70:449-53.
- [Google Scholar]
- Fluorescence in situ hybridization in diagnostic cytology. Hum Pathol. 2007;38:1137-44.
- [Google Scholar]
- ImmunoCyt and cytokeratin 20 immunocytochemistry as adjunct markers for urine cytologic detection of bladder cancer: A prospective study. Anal Quant Cytol Histol. 2010;32:45-52.
- [Google Scholar]
- Cytokeratin 20 as an immunocytochemical marker for detection of urothelial carcinoma in atypical cytology: Preliminary retrospective study on archived urine slides. Cancer Detect Prev. 2001;25:202-9.
- [Google Scholar]
- Mucin 7 and cytokeratin 20 as new diagnostic urinary markers for bladder tumor. J Urol. 2003;169:86-9.
- [Google Scholar]
- Immunohistochemical expression of CK20, p53, and Ki-67 as objective markers of urothelial dysplasia. Mod Pathol. 2003;16:187-91.
- [Google Scholar]
- Expression of cytokeratin 20 in urinary cytology of patients with bladder carcinoma. Cancer. 1998;82:349-54.
- [Google Scholar]
- Utility of a dual immunostain cocktail comprising of p53 and CK20 to aid in the diagnosis of non-neoplastic and neoplastic bladder biopsies. Diagn Pathol. 2009;4:35.
- [Google Scholar]
- Expression of cytokeratin 20 in urine cytology smears: A potential marker for the detection of urothelial carcinoma. Cytopathology. 2007;18:84-6.
- [Google Scholar]
- Which urine marker test provides more diagnostic value in conjunction with standard cytology-immunocyt/uCyt+or cytokeratin 20 expression. Diagn Pathol. 2009;4:20.
- [Google Scholar]
- Immunostaining of cytokeratin 20 in cells from voided urine for detection of bladder cancer. J Urol. 2000;164:1922-5.
- [Google Scholar]
- Urine cytology and adjunct markers for detection and surveillance of bladder cancer. Am J Transl Res. 2010;2:412-40.
- [Google Scholar]
- Cytokeratin 20 as an objective marker of urothelial dysplasia. Br J Urol. 1996;78:870-5.
- [Google Scholar]
- p53 protein and Ki-67 overexpression in urothelial dysplasia of bladder. Appl Immunohistochem Mol Morphol. 2002;10:327-31.
- [Google Scholar]
- Expression of cytokeratin 20 redefines urothelial papillomas of the bladder. Lancet. 1999;353:974-7.
- [Google Scholar]
- Cytokeratin 7 and cytokeratin 20 expression in epithelial neoplasms: A survey of 435 cases. Mod Pathol. 2000;13:962-72.
- [Google Scholar]
- Relationship of cytokeratin 20 and CD44 protein expression with WHO/ISUP grade in pTa and pT1 papillary urothelial neoplasia. Mod Pathol. 2000;13:1315-23.
- [Google Scholar]
- Comparison of the WHO/ISUP classification and cytokeratin 20 expression in predicting the behavior of low-grade papillary urothelial tumors. World/Health Organization/Internattional Society of Urologic Pathology. Mod Pathol. 2001;14:267-72.
- [Google Scholar]
- Cytokeratin 20 and Ki-67 to distinguish carcinoma in situ from flat non-neoplastic urothelium. Appl Immunohistochem Mol Morphol. 2006;14:260-5.
- [Google Scholar]
- Utility of cytokeratin 20 and Ki-67 as markers of urothelial dysplasia. Pathol Int. 2005;55:248-54.
- [Google Scholar]
- Immunophenotype of high-grade prostatic adenocarcinoma and urothelial carcinoma. Mod Pathol. 2000;13:1186-91.
- [Google Scholar]
- Potential utility of uroplakin III, thrombomodulin, high molecular weight cytokeratin, and cytokeratin 20 in noninvasive, invasive, and metastatic urothelial (transitional cell) carcinomas. Am J Surg Pathol. 2003;27:1-10.
- [Google Scholar]
- Cytokeratin-20 immunocytology in voided urine exhibits greater sensitivity and reliability than standard cytology in the diagnosis of transitional cell carcinoma of the bladder. Urology. 2005;66:536-41.
- [Google Scholar]
- Allelic loss of chromosome 17p distinguishes high grade from low grade transitional cell carcinomas of the bladder. Cancer Res. 1990;50:7081-3.
- [Google Scholar]
- Identification of p53 gene mutations in bladder cancers and urine samples. Science. 1991;252:706-9.
- [Google Scholar]
- Expression of mutant p53, c-erbB-2 and the epidermal growth factor receptor in transitional cell carcinoma of the human urinary bladder. Br J Cancer. 1991;63:967-70.
- [Google Scholar]
- p53 immunohistochemistry in transitional cell carcinoma and dysplasia of the urinary bladder correlates with disease progression. Br J Cancer. 1993;68:1029-35.
- [Google Scholar]
- Histologic grading of noninvasive papillary urothelial tumors: Validation of the 1998 WHO/ISUP system by immunophenotyping and follow-up. Am J Clin Pathol. 2004;121:679-87.
- [Google Scholar]
- Diagnostic value of fibronectin and mutant p53 in the urine of patients with bladder cancer: Impact on clinicopathological features and disease recurrence. Med Oncol. 2010;27:1286-94.
- [Google Scholar]
- Does p53 immunostaining improve diagnostic accuracy in urine cytology? Diagn Cytopathol. 1997;17:436-9.
- [Google Scholar]
- Multifocal transitional cell carcinoma of the bladder and upper urinary tract: Molecular screening of clonal origin by characterizing CD44 alternative splicing patterns. J Urol. 2004;172:1127-9.
- [Google Scholar]
- Noninvasive diagnosis of bladder carcinoma by enzyme-linked immunosorbent assay detection of CD44 isoforms in exfoliated urothelia. Clin Cancer Res. 2000;6:2381-92.
- [Google Scholar]
- Expression of CD44 standard and variant-v6 proteins in transitional cell bladder tumours and their relation to prognosis during a long-term follow-up. J Pathol. 1998;186:157-64.
- [Google Scholar]
- Expression of the CD44 cell adhesion molecule in urinary bladder transitional cell carcinoma. Mod Pathol. 1996;9:854-60.
- [Google Scholar]
- Focal loss of CD44 variant protein expression is related to recurrence in superficial bladder carcinoma. Am J Pathol. 1999;155:1427-32.
- [Google Scholar]
- A review on the current state of urine cytology emphasizing the role of fluorescence in situ hybridization as an adjunct to diagnosis. Cancer Cytopathol. 2010;118:175-83.
- [Google Scholar]
- Multiprobe FISH for enhanced detection of bladder cancer in voided urine specimens and bladder washings. Am J Clin Pathol. 2001;116:79-86.
- [Google Scholar]
- A comparison of cytology and fluorescence in situ hybridization for the detection of urothelial carcinoma. J Urol. 2000;164:1768-75.
- [Google Scholar]
- Multitarget fluorescence in situ hybridization assay detects transitional cell carcinoma in the majority of patients with bladder cancer and atypical or negative urine cytology. J Urol. 2003;169:2101-5.
- [Google Scholar]
- Clinical evaluation of a multi-target fluorescent in situ hybridization assay for detection of bladder cancer. J Urol. 2002;168:1950-4.
- [Google Scholar]
- Reflex UroVysion testing of bladder cancer surveillance patients with equivocal or negative urine cytology: A prospective study with focus on the natural history of anticipatory positive findings. Am J Clin Pathol. 2007;127:295-301.
- [Google Scholar]




