


Translate this page into:
Collagenous spherulosis: An interesting cytological finding in breast lesion
*Corresponding author
-
Received: ,
Accepted: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Collagenous spherulosis (CS) is a rare and interesting entity associated with benign breast lesions. CS is an incidental finding picked up only on 0.2% of cytology specimen. Typically cytologically of CS of breast consists of central spherical hyaline spherule surrounded by myoepithelial cells. The central hyaline spherule has been found to be basement membrane material histochemically and immunohistochemically. The importance of recognizing CS of breast lies in the fact that similar hyaline globules can occur in adenoid cystic carcinoma of the breast (ACCB). The two lesions need to be differentiated on cytology failing which inappropriate treatment can be given for either of the two lesions. We present here a case of CS associated with benign breast lesion and a case of ACCB to describe their cytological features and key points to differentiate them cytologically.
Keywords
Adenoid cystic carcinoma
collagenous spherulosis
hyaline spherule

INTRODUCTION
Collagenous spherulosis (CS) of the breast is an interesting finding in breast lesion which results from the accumulation of basement membrane material in the form of eosinophilic spherules.[1] Breast CS is an incidental finding which may occur in isolation or more commonly it occurs in association with benign proliferative breast lesions.[1] The main concern regarding breast CS is that it may be misinterpreted as adenoid cystic carcinoma of the breast (ACCB).[1] ACCB is characterized by hyaline globules which have a morphology similar to CS. We described a case of CS associated with benign breast disease and a case of ACCB to compare and to highlight the differences between two entities on breast cytology.
CASE REPORT
A 25-year-old female presented with a painless and mobile lump in breast measuring 2.5 cm × 2.5 cm. Aspiration cytology of the lump revealed moderately cellular smears comprising of few branching fragments of benign ductal epithelial cells intimately mixed with spherical acellular homogenous hyaline globules [Figure 1a and b]. A few dispersed bare, bipolar cells were also seen in the background. A cytological diagnosis of CS associated with benign proliferative breast disease was given.
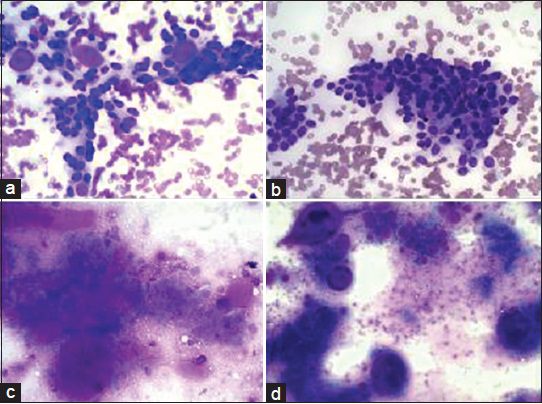
- (a and b): Aspiration cytology of collagenous spherulosis reveal moderately cellular smears comprising of few branching fragments of benign ductal epithelial cells intimately mixed with spherical acellular homogenous hyaline globules (Giemsa, ×40). (c and d) Aspiration smears from adenoid cystic carcinoma of breast reveal cellular smears composed of epithelial cells and acellular basement material. The epithelial cells are small and basaloid forming cohesive, spherical, and tri-dimensional structures with central core of acellular homogenous basement membrane substance (Giemsa, ×40)
A 59-year-old female presented with a lump in the upper-outer quadrant of left breast measuring 5 cm × 5 cm. The magnetic resonance imaging revealed a heterogeneous noninfiltrating lesion in the left breast. The axilla was clear. The fine-needle aspiration cytology from the left breast lump revealed cellular smears composed of epithelial cells and acellular basement material. The epithelial cells were small and basaloid forming cohesive, spherical, and tri-dimensional structures with a central core of acellular homogenous basement membrane substance [Figure 1c and d]. A cytological diagnosis of ACCB was given. The patient underwent left mastectomy. Mastectomy specimen revealed a 4.5 cm × 4.5 cm × 3.5 cm lesion in the upper-outer quadrant of the left breast. Microscopic examination revealed tumor cells arranged in solid nests, proliferating glands, and cylideromatous differentiation containing eosinophilic basement membrane-like material and basophilic secretions. The areas of cribriform pattern were also seen in the desmoplastic stroma. All resection margins, nipple, and areola, were free from tumor invasion. The histopathology confirmed the cytological diagnosis of ACCB.
DISCUSSION
CS of the breast was first described as an entity by Clement and Young in 1987.[1] CS of the breast is a rare benign lesion with reported incidence of <1% in excisional specimens and <0.2% in cytology material.[2] The reported incidence of CS is low because of lack of awareness of this entity among cytopathologists. CS has been frequently seen in association with benign breast lesions such as sclerosing adenosis, radial scar, intraductal papilloma, fibroadenoma, adenomyoepithelioma, and atypical ductal hyperplasia.[23]
CS is characterized by the presence of acellular eosinophilic spheres varying in diameter from 20 to 100 nm.[1] Ultrastructurally, the spherules are fibrillar either arranged in star-shaped configuration or a laminar concentric appearance with central hyaline globule.[1] Histochemically, spherules in CS are composed of type IV collagen consisting of laminin, fibronectin, and heparin sulfate.[4] Thus, the spherules take up connective tissue stains blue with trichrome stain, pink-red with van Gieson, black with reticulin, and variably positive with PAS and Alcian stain. The source of the basement membrane material is the myoepithelial cells which surround the spherules of CS.[5] Immunohistochemistry (IHC) confirms that the cells surrounding the spherules are myoepithelial cells and show positivity for actin, calponin, S-100, p63, and smooth muscle myosin.[6]
A malignant breast tumor which may be confused with CS on cytology is ACCB. ACCB is a rare salivary gland-like tumor of the breast which makes up <0.1% of all breast tumors.[7] The cytology of ACCB is highly cellular, comprising of small, uniform, monotonous cells having very little cytoplasm, smooth chromatin and few, if any, nucleoli. Naked nuclei of these small cells are present in the background, and are a very little admixture of typical benign duct cell groups.[8] Extracellular metachromatic spheres are required for the diagnosis. The extracellular material has been found to be basement membrane material consisting of type IV collagen. Cytologically, CS of the breast show monolayered clusters of cells with little branching architecture, and the cells have a low nuclear/cytoplasmic ratio. In contrast, ACCB is composed of syncytial, multilayered, branching clusters of cells having a high nuclear/cytoplasmic ratio. In addition, the acellular spherules of CS of the breast are often surrounded by only a single layer of nuclei, whereas the spherules of ACCB are typically surrounded by several layers.[59]
It is important for the cytopathologists to differentiate between benign CS and ACCB because the management for these two entities is totally different. The easiest way to make a distinction is by strict adherence to the requirement of the presence of both the basaloid and eosinophilic cell types for a diagnosis of ACCB.[10] However, in difficult situations an open biopsy is suggested.[11] IHC is also helpful in differentiating these two entities. Smooth muscle myosin heavy chain and calponin are uniformly and strongly positive in CS and negative in ACCB. C-kit (CD117) is a sensitive marker of ACCB, which is not expressed in CS.[6]
CS is an infrequently reported entity mainly because of inability to recognize the entity. However, it is essential for cytopathologists to recognize this entity and avoid a false positive diagnosis of malignancy. The failure to recognize CS as a benign lesion may result in overestimation of a patient's subsequent risk of invasive cancer, or at worst may cause inappropriate treatment on the basis of this diagnosis.
COMPETING INTERESTS STATEMENT BY ALL AUTHORS
All authors declare no competing interests.
AUTHORSHIP STATEMENT BY ALL AUTHORS
All authors of this manuscript declare that they qualify for authorship as defined by the ICMJE. All the authors are responsible for the conception of this study, have participated in its design and coordination, and helped to draft the manuscript. All authors have read and approved the final manuscript.
ETHICS STATEMENT BY ALL AUTHORS
Since this is a case report without identifiers, our institution does not require approval from the Institutional Review Board.
LIST OF ABBREVIATIONS (In alphabetic order)
ACCB - Adenoid Cystic Carcinoma of the Breastm
CS - Collagenous Spherulosis
IHC - Immunohistochemistry
EDITORIAL/PEER-REVIEW STATEMENT
To ensure the integrity and the highest quality of CytoJournal publications, the review process of this manuscript was conducted under a double-blind model (authors are blinded for reviewers and vice versa) through automatic online system.
Available FREE in open access from: http://www.cytojournal.com/text.asp?2015/12/1/25/170725
REFERENCES
- Collagenous spherulosis of breast: Morphologic study of 59 cases and review of the literature. Am J Surg Pathol. 2006;30:20-7.
- [Google Scholar]
- Collagenous spherulosis associated with adenomyoepithelioma of the breast: A case report. Acta Cytol. 2010;54:314-8.
- [Google Scholar]
- Collagenous spherulosis of breast: Diagnosis by FNAB with review of literature. Indian J Pathol Microbiol. 2000;43:131-4.
- [Google Scholar]
- Collagenous spherulosis. Report of a case with diagnosis by fine needle aspiration biopsy with immunocytochemical and ultrastructural observations. Acta Cytol. 1993;37:3-9.
- [Google Scholar]
- Immunophenotypic overlap between adenoid cystic carcinoma and collagenous spherulosis of the breast: Potential diagnostic pitfalls using myoepithelial markers. Mod Pathol. 2006;19:1351-7.
- [Google Scholar]
- Adenoid cystic carcinoma of the breast: Diagnosis by fine-needle aspiration. Diagn Cytopathol. 1993;9:184-7.
- [Google Scholar]
- Diagnosis of collagenous spherulosis of the breast by fine needle aspiration cytology. A report of two cases. Acta Cytol. 1993;37:725-8.
- [Google Scholar]
- A case of mucinous spherulosis of the breast diagnosed retrospectively in FNA material. Diagn Cytopathol. 2006;34:626-30.
- [Google Scholar]




