


Translate this page into:
Comparative study of ProEx C immunocytochemistry and UroVysion fluorescent in-situ hybridization assays on urine cytology specimens
-
Received: ,
Accepted: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
Detection of urothelial carcinoma (UC) by urine cytology can be challenging. Recently, ProEx C has been studied as a marker to improve detection of UC. ProEx C is an assay targeting expression of topoisomerase IIa and minichromosome maintenance protein-2 and is currently utilized to assist in diagnoses of the gynecological specimens. In this study, we compared the utility of ProEx C and UroVysion in urine specimens.
Materials and Methods:
Twenty-seven urine specimens with UroVysion assay analysis and surgical biopsy follow-up were selected. The smears were stained with ProEx C. ProEx C and UroVysion assay results were separated into two categories based on surgical biopsy follow-up (benign or neoplastic). Surgical biopsy diagnoses were used as the gold standard for comparative evaluation of the two assays. The surgical follow-up was 9 benign, 2 low grade, and 16 high grade UCs.
Results:
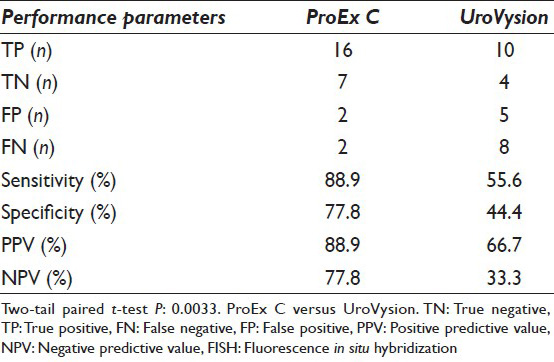
The sensitivity was 88.9% for ProEx C and 55.6% for UroVysion, while the specificity was 77.8% for ProEx C and 44.4% for UroVysion. Positive predictive value was 88.9% for ProEx C and 66.7% for UroVysion. Negative predictive value was 77.8% and 33.3% for ProEx C and UroVysion, respectively. Using the two-tailed paired t-test, P value of 0.033 was obtained when ProEx C stain was compared with the UroVysion assay.
Conclusion:
ProEx C immunocytochemistry has a more favorable performance than fluorescent in-situ hybridization with a significant difference between the two assays using paired two-tail t-test (P = 0.0033).
Keywords
Cytology
ProEx C
urine
urothelial carcinoma
UroVysion

INTRODUCTION
Urothelial carcinoma (UC) is the sixth most prevalent cancer among males and females. It is the most common malignancy of the lower urinary tract, with an estimated 15,210 annual deaths from the disease.[1] Detection of UC by urine cytology is often challenging and can be subjective. Cystoscopy and surgical biopsy are the diagnostic reference standard but are invasive and expensive. On the other hand, urine cytology has the benefit of being safe and inexpensive. But due to the nature of the specimens, the cellular morphology may be affected by degenerative and/or reactive processes and sometimes confounded by infections, leading to atypia indistinguishable from a neoplastic lesion.[23] To assist with the evaluation of “atypical urothelial cells (AUCs),” several ancillary tests and adjunct assays have been employed to improve the sensitivity of detecting UCs in urine cytology. These ancillary studies include immunocytochemical (IHC) stains and assays such as CK20, Ki67, hTERT, UroVysion™, and ImmunoCyt/uCyt™.[45678] UroVysion™ fluorescent in-situ hybridization (FISH) assay is a commonly used ancillary test, which uses fluorescent probes to detect hyperploidy of chromosomes 3, 7, and 17, and loss of P16 gene on the 9p21 locus. In a meta-analysis by Hajdinak, UroVysion had a sensitivity of 72% and a specificity of 83%.[9] Recently, ProEx C by IHC has been introduced as an adjunct test.
ProEx C is a cocktail of antibodies against minichromosome maintenance protein 2 (MCM2) and topoisomerase IIa protein (TOP2A). MCM2 and TOP2A are overexpressed in the cell nucleus during aberrant S-phase induction in neoplastic cells, although they are also expressed only in the basal/parabasal cells of normal and hyperactive epithelium. This antibody cocktail was originally developed to assess squamous dysplasia in gynecologic specimens.[1011] In previously reported studies, MCM2 and MCM5 had been utilized as prognostic indicators of recurrence in stage Ta/T1 UCs.[712] These and other studies[71012] became the basis for the introduction of ProEx C utilization as an adjunct diagnostic test for UC in urine cytology.[13]
A comparative study of ProEx C versus ImmunoCyt/uCyt has already been carried out.[14] The current study compares the assay performances of ProEx C and UroVysion, the latter one of the widely used ancillary tests on urine samples.
MATERIALS AND METHODS
Case selection
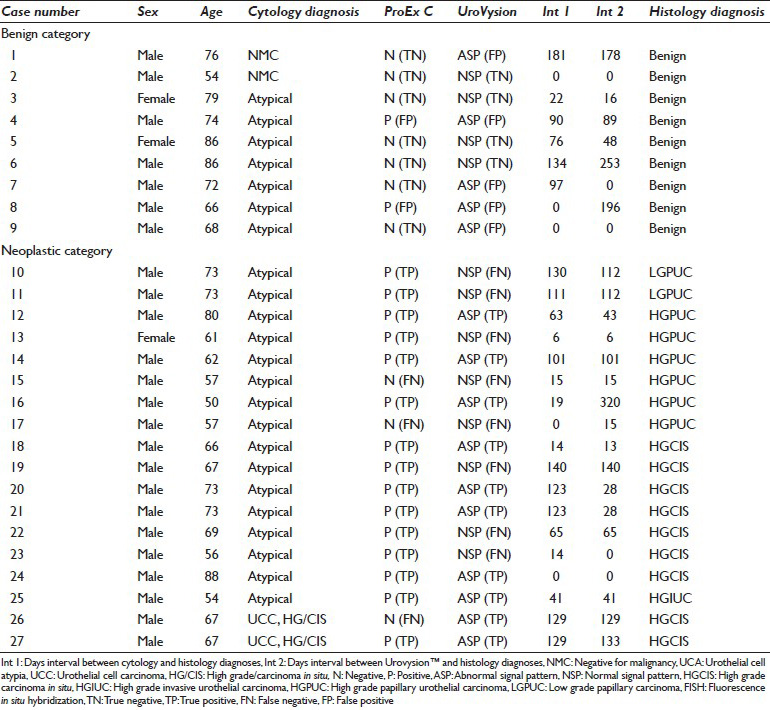
This study was approved by the Institutional Review Board in our institution (IRB# 09-07-108-01). This retrospective study investigated the patients with urine cytology reports who had surgical biopsy follow-up results within 1 year of cytological examination for the period of January 2006 to December 2009. Cases that had concomitant ProEx C by IHC and UroVysion by FISH assay were selected for this study. The pertinent patients’ demographic data, including the intervals between the cytological and histopathologic diagnoses along with the test results, are displayed in Table 1.
UroVysion™ fluorescent in-situ hybridization assays
UroVysion™ Bladder Cancer Kits were obtained from Abbott Laboratories (1300 E. Touhy Ave., Des Plaines, IL, USA). Each kit contained three alpha-satellite repeat sequences or chromosome enumeration probes (CEP) for chromosome-3 (SpectrumRed), chromosome-7 (SpectrumGreen), and chromosome-17 (SpectrumAqua). In the assay, the three CEP hybridize to the centromeric regions of chromosomes 3, 7, and 17, respectively. In addition, a unique sequence locus specific identifier probe (SpectrumGold) was included to detect P16 gene on p21 locus of chromosome 9. The urinary specimens were processed for the FISH assay according to the Food and Drug Administration (FDA) approved methodology as described in the product insert. An epifluorescence microscope equipped with appropriate excitation and barrier filters was used to visualize and record the signals. In this process, nuclear DAPI and the respective probe signal images were individually photographed for accurate signal counting then the acquired images were combined to form a complete image of the cells. According to the FDA criteria, the normal diploid urothelial cells have two signals for each chromosome [Figure 1]. An abnormal FISH assay for a suspected urothelial neoplasia would require a minimum of four cells with polysomy of at least two of the four chromosomes [Figure 2] or a minimum of 12 cells with homozygous loss of P16 genes when a minimum of 25 large atypical cells were examined. Umbrella cells were excluded for evaluation.[15]
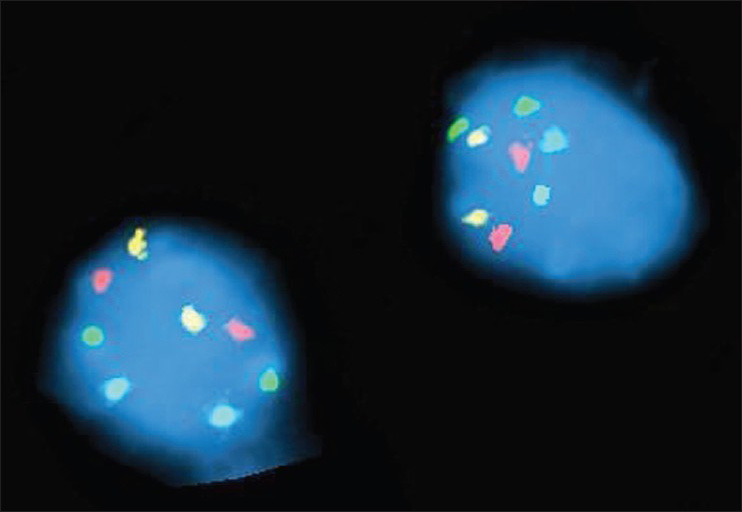
- An example of UroVysion fluorescent labeling in normal cells. Fluorescent in-situ hybridization analysis with probe panel (four probes) which includes alpha satellite probes specific for chromosomes 3, 7, and 17, and locus specific probe at the 9p21 region was performed. These studies showed a normal signal pattern and no evidence of polysomy in the 25 nuclei examined
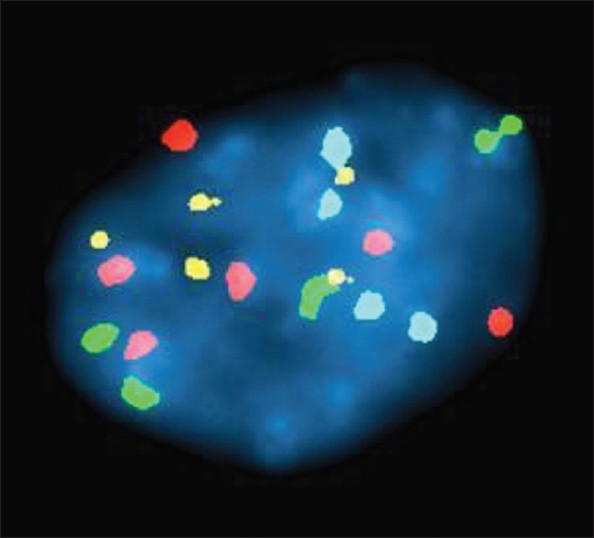
- An example of UroVysion fluorescent labeling in an abnormal cell. These studies showed an abnormal signal pattern (aneusomy of chromosomes 3, 7, or 17, or deletion of the 9p21 locus) in 17 of the cells analyzed magnification. The follow-up surgical biopsy showed high grade urothelial carcinoma [case #27, Table 1]
ProEx C immunostaining
ProEx C™ antibody cocktail (BD ProEx C IHC), BD SureDetect detection reagents kit, and BD SureDetect SiHa Cell control slides were obtained from BD Diagnostics-TriPath (Burlington, NC, USA). The staining procedure was performed manually by following the published procedure in the manufacturer product insert. Archived ThinPrep Pap-stained slides were immersed for a week to remove the glass coverslips. Removal of the mounting media was performed under standard protocol using xylene rinses. The slides were then rehydrated with a series of graduated ethanol dilutions. Destaining was then accomplished in 1% hydrochloric acid/70% ethanol for 5 min, and then washed with phosphate-buffered saline solution. Subsequently, the slides were restained with ProEx C using manual IHC technique along with positive and negative controls (SiHa cells). The primary antibody of ProEx C (a cocktail of mouse monoclonal anti-MCM2 and anti-TOP2A) was dispensed onto slides and incubated for 30 min and rinsed off. Minimal artifacts and/or loss of cellularity were encountered due to destaining and restaining. ProEx C scoring was recorded as positive if at least one morphologically AUC displayed positive nuclear staining as described previously.[13] An example of the ProEx C stain in a case of high-grade UC [case #27, Table 1] is shown in Figure 3.
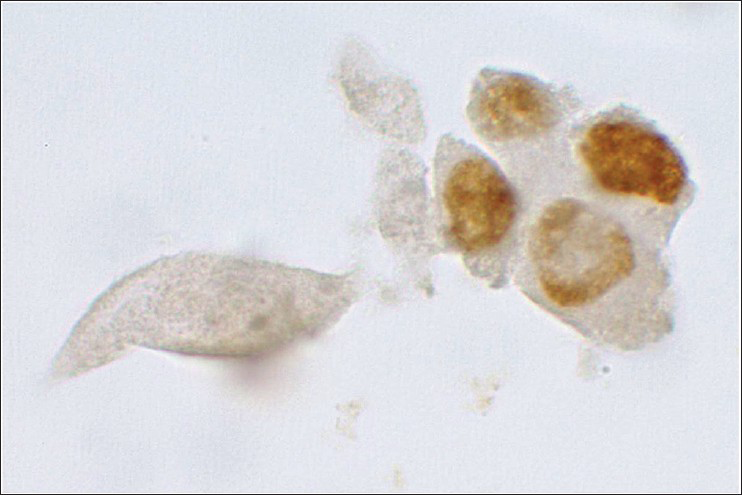
- An example of positive ProEx C staining of malignant urothelial cells (case #27, Table 1). In this case, ProEx C immunohistochemical stain exhibits intense nuclear reaction in >1 cytologically atypical cell (cytology, ×100)
Study design
ProEx C and UroVysion assay results were separated into two categories based on surgical biopsy follow-up; benign and neoplastic [Table 1]. The Neoplastic category included low-grade papillary UC (LGPUC), high-grade papillary UC (HGPUC), high-grade carcinoma in-situ (HGCIS), and high-grade invasive UC (HGIUC). The histopathology diagnoses were used as the gold standard for comparative evaluation of the two assays. Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were determined for both assays.[16] Assay performances were calculated for combined benign and neoplastic categories [Table 2]. Paired two-tail t-test was employed to compare the two assays using the lists of the individual patients as indicated in Table 2. P value of 0.05 or less was considered a significant difference between the two compared assays. Office Excel 2010 (Microsoft, Redmond, Washington, USA) was used for data tabulation and statistical analyses.
RESULTS
A total of 27 cases, with a median age of 70 years (54–86), were selected for the current study using the criteria described in the materials and methods section. The overall demographic data and the assay test results are summarized in Table 1. There were 24 men and 3 women. The cytology diagnoses were negative for malignancy in 2 [#1 and 2, Table 1], AUCs in 23 [#3–25, Table 1], and urothelial cell carcinoma, HG/CIS in 2 [#26 and 27, Table 1] cases. The interval ranges between cytology and histology diagnoses were 0–181 days. The interval ranges between the FISH assay and histology diagnoses were 0–320 days. The histopathologic follow-up diagnoses were benign in 9 [#1–9, Table 1], LGPUC in 2 [#10 and 11, Table 1], and high grade urothelial neoplasia in 16 [#12–27, Table 1] patients. The test performances of the two assays among the 27 cases are shown in Table 2. The sensitivity was 88.9% for ProEx C and 55.6% for UroVysion, while the specificity was 77.8% for ProEx C and 44.4% for UroVysion. PPV was 88.9% for ProEx C and 66.7% for UroVysion. NPV was 77.8% and 33.3% for ProEx C and UroVysion respectively. Across the board, ProEx C had more favorable performance values than the FISH assay with a significant difference between the two assays by two-tail paired t-test (P = 0.0033).
Benign category
There were nine patients [#1–9, Table 1] with benign histology follow-up of which two were diagnosed as benign by cytology while the remaining seven were called “atypical.” In this category, ProEx C and FISH assays had two and five false positive results respectively. The difference between the two assays in this category (P = 0.0805) was due to higher false positive reactions of the FISH assay.
Neoplastic category
There were 18 patients in this category. The histopathology diagnoses were LGPUC [#10–11, Table 1] for two and high-grade urothelial cancers for 16 patients [Table 1]. The high grade neoplastic lesions included eight HGPUC [#12–17, Table 1], seven HGCIS [#18–24 and 26–27, Table 1], and one HGIUC [#25, Table 1]. ProEx C detected 16 of 18 patients as true positive while for the FISH assay there were only 10 true positives. An example of a true positive case by the FISH and ProEx C IHC assays is shown in Figures 2 and 3 [#27, Table 1] respectively. There was a significant difference between the two assays in this category (P = 0.0096) due to a higher true positive reactivity of ProEx C.
DISCUSSION
To the best of our knowledge, this is the first study comparing the performance of ProEx C IHC with UroVysion™ FISH assay as adjunct tests in urine cytology. At the outset, the ProEx C assay is superior to UroVysion and for that matter to uCyt[14] as an ancillary test for detection of UCs. The sensitivity and specificity for the ProEx C are 89–78% respectively as opposed to 56% and 44% for UroVysion in this series [Table 2]. The ProEx C assay performance for the current series is in concordance with the previously published studies.[1314]
The two most common ancillary tests currently used on exfoliative urothelial cells are uCyt and UroVysion where the latter is more commonly employed.[1718] These two assays are generally processed and analyzed by others, rather than the primary cytotechnologists and/or cytopathologists imposing a disadvantage for the two assays. These tests are time-consuming and require trained and certified personnel. There is a wide range of variation in the test performance of the FISH assay in literature. For example, the sensitivity of UroVysion test ranges from 39% to 97% and the specificity from 21% to 100%.[1920] In addition, tetraploidy factors in the variations of the assay results as experienced by some investigators.[212223] A meta-analysis study performed by Hajdinak in 2008 showed a sensitivity of 72% and a specificity of 83% for the FISH assay.[9] Sullivan et al. in a comparative study of ImmunoCyt/uCyt and UroVysion in 2009, have reported a more favorable sensitivity for ImmunoCyt/uCyt than UroVysion.[17]
In the original published study, utilizing ProEx C in urinary cytology, ProEx C has its most favorable results in the setting of definitive benign and malignant cytologic specimens for predicting both LGUC and HGUC.[13] In a follow-up comparative study in the AUC setting, ProEx C has also exhibited a superior specificity when compared to ImmunoCyt/uCyt.[14] This particular study has also shown that ProEx C has a higher sensitivity for detection of HGUC than LGPUC.[14] On histological sections of the urothelial neoplasia, ProEx C staining involves the full thickness of the cancerous epithelium in HGUC in contrast to LGPUC where the reaction is focal and closer to the basal layers.[24] Therefore, the positive cells may not reach the surface for exfoliation into the urinary samples which account for the lower sensitivity of the assay in LGPUC.[24]
The current study shows that ProEx C assay performance parameters are comparable to those previously published.[1314] Due to the lower number of the cases in this series, we did not specifically compare the LGUC and HGUC performance assay. As a whole, ProEx C displays a higher sensitivity than UroVysion for identifying UCs (88.9–55.6% respectively). In addition, much higher PPV (88.9%) and NPV (77.8%) were observed for ProEx C than those for UroVysion that were at 64.3–30.8% respectively [Table 2].
Aside from the assay performance, ProEx C is a more advantageous ancillary test than UroVysion or ImmunoCyt/uCyt since urinary cytology slides are examined alongside the ProEx C stain by the same cytotechnologists and pathologists using their own light microscopes, requiring no special expertise or additional certification. At the outset, the ProEx C is a comprehensive assay, which is simpler and more cost-effective.
CONCLUSION
This study further emphasizes that ProEx C has superior assay performances than UroVysion and/or ImmunoCyt/uCyt.[14] ProEx C would serve well as a second adjunct marker for the analysis of urothelial specimens. Although the findings in the previously published study, as well as the current series, highly favor ProEx C as an ancillary test in urine cytology.[1324] future works using much larger series are needed to further crystalize the current findings.
COMPETING INTERESTS
The authors declare that they have no competing interests.
AUTHORS CONTRIBUTIONS
SC, Pathology resident, reviewed all the data, participated in cytological evaluation, and manuscript review. ES, Cytotechnology student, collected all the data, and manuscript review. JYR, cytological evaluation and manuscript review. ML, reviewed the data and manuscript review. NAM, Conceptual organization, cytological evaluation, and manuscript review and editing.
ETHICS STATEMENT BY ALL AUTHORS
This study was approved by the Institutional Review Board of the University of California, Los Angeles. This work has been cleared through the IRB at UCLA Medical Center.
EDITORIAL/PEER-REVIEW STATEMENT
To ensure the integrity and highest quality of CytoJournal publications, the review process of this manuscript was conducted under a double blind model (authors are blinded for reviewers and vice versa) through automatic online system.
ACKNOWLEDGMENTS
This study was supported by a Translational Research Fund grant from the UCLA Department of Pathology and Laboratory Medicine. The authors are grateful to Mr. Jin Yusheng for his invaluable assistance in IHC staining of the slides. There is also no related conflict of interest by the authors. This work was presented as a poster in the Cytopathology section at the 103rd United States and Canadian Academy of Pathology annual meeting in San Diego, California, on March 5, 2014.
REFERENCES
- Cancer treatment and survivorship statistics, 2012. CA Cancer J Clin. 2012;62:220-41.
- [Google Scholar]
- Urine. In: DeMay RM, ed. The Art and Science of Cytopathology. Chicago: ASCP; 2012. p. :435-77.
- [Google Scholar]
- Relationship of cytokeratin 20 and CD44 protein expression with WHO/ISUP grade in pTa and pT1 papillary urothelial neoplasia. Mod Pathol. 2000;13:1315-23.
- [Google Scholar]
- Fluorescence in situ hybridization in diagnostic cytology. Hum Pathol. 2007;38:1137-44.
- [Google Scholar]
- Immunohistochemical detection of hTERT in urothelial lesions: A potential adjunct to urine cytology. Cytojournal. 2006;3:18.
- [Google Scholar]
- Mcm2 predicts recurrence hazard in stage Ta/T1 bladder cancer more accurately than CK20, Ki67 and histological grade. Br J Cancer. 2007;96:1711-5.
- [Google Scholar]
- ImmunoCyt and cytokeratin 20 immunocytochemistry as adjunct markers for urine cytologic detection of bladder cancer: A prospective study. Anal Quant Cytol Histol. 2010;32:45-52.
- [Google Scholar]
- UroVysion FISH test for detecting urothelial cancers: Meta-analysis of diagnostic accuracy and comparison with urinary cytology testing. Urol Oncol. 2008;26:646-51.
- [Google Scholar]
- BD ProEx C: A sensitive and specific marker of HPV-associated squamous lesions of the cervix. Am J Surg Pathol. 2008;32:899-906.
- [Google Scholar]
- The role of deeper levels and ancillary studies (p16(Ink4a) and ProExC) in reducing the discordance rate of Papanicolaou findings of high-grade squamous intraepithelial lesion and follow-up cervical biopsies. Cancer. 2009;117:157-66.
- [Google Scholar]
- Prognostic value of MCM2 immunoreactivity in stage T1 transitional cell carcinoma of the bladder. Eur Urol. 2003;43:138-45.
- [Google Scholar]
- ProEx C as an adjunct marker to improve cytological detection of urothelial carcinoma in urinary specimens. Cancer Cytopathol. 2013;121:320-8.
- [Google Scholar]
- Comparative evaluation of ProEx C and ImmunoCyt/uCyt assays in atypical urine cytology. Arch Pathol Lab Med. 2014;138:1215-22.
- [Google Scholar]
- Superficial urothelial (umbrella) cells. A potential cause of abnormal DNA ploidy results in urine specimens. Anal Quant Cytol Histol. 2000;22:411-5.
- [Google Scholar]
- Principles of laboratory medicine. In: Howanitz JH, Howanitz PJ, eds. Laboratory Medicine. Test Selection and Interpretation. New York: Churchill Livingston; 1991. p. :1-10.
- [Google Scholar]
- Comparison of ImmunoCyt, UroVysion, and urine cytology in detection of recurrent urothelial carcinoma: A “split-sample” study. Cancer. 2009;117:167-73.
- [Google Scholar]
- Diagnosis of genito-urinary tract cancer by detection of minichromosome maintenance 5 protein in urine sediments. J Natl Cancer Inst. 2002;94:1071-9.
- [Google Scholar]
- Reflex UroVysion testing in suspicious urine cytology cases. Cancer. 2009;117:7-14.
- [Google Scholar]
- Multiprobe FISH for enhanced detection of bladder cancer in voided urine specimens and bladder washings. Am J Clin Pathol. 2001;116:79-86.
- [Google Scholar]
- Multi-target fluorescence in situ hybridization in bladder washings for prediction of recurrent bladder cancer. Int J Cancer. 2006;119:1660-5.
- [Google Scholar]
- Exclusion of the uniform tetraploid cells significantly improves specificity of the urine FISH assay. Diagn Cytopathol. 2013;41:218-25.
- [Google Scholar]
- Utility of ProEx C in the histologic evaluation of the neoplastic and nonneoplastic urothelial lesions. Hum Pathol. 2013;44:2509-17.
- [Google Scholar]




