


Translate this page into:
Diagnostic utility of conventional and liquid-based cytology in the management of thyroid lesions; an institutional experience

*Corresponding author: Rohit Sharma, Assistant Professor, Department of Pathology, Andaman and Nicobar Islands Institute of Medical Sciences (ANIIMS), Port Blair, Andaman and Nicobar Islands, India. rohitsjh@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Sharma R, Zaheer S, Ahluwalia C. Diagnostic utility of conventional and liquid based cytology in the management of thyroid lesions; an institutional experience. CytoJournal 2022;19:36.
Abstract
Objectives:
Liquid-based cytology (LBC) is becoming a useful method in evaluating both gynecological and nongynecological preparations. Many studies have been conducted these days to see the quality of LBC in diagnosing thyroid lesions and its role is yet to be standardized. This study has been done to pick the cytomorphological features of thyroid lesions on LBC and to compare them with the conventional cytology of these lesions.The objective of the study is to evaluate the efficacy of thyroid fine-needle aspiration cytology processed by LBC as compared to conventional smears.
Material and Methods:
A prospective study has been done on 53 cases of thyroid lesions using standard conventional and LBC techniques.
Results:
In most of the cases, the cytological features are similar in conventional cytology smears and LBC, but the colloid film and the lymphocytic component show a clear picture on direct smears, whereas nuclear and cytoplasmic details are better evaluated in LBC slides. The preservative solution used in LBC could be efficiently used for the application of immunocytochemical and molecular techniques.
Conclusion:
LBC does not represent as a valid alternative to conventional cytology but it can be considered as a diagnostic utility process especially due to the possibility of applying additional techniques which enhance the efficacy of the cytological diagnosis of thyroid lesions.
Keywords
Liquid-based cytology
Thyroid
Fine needle aspiration cytology

INTRODUCTION
Fine-needle aspiration cytology (FNAC) is a fast, simple, and cost-effective preliminary procedure where cells are obtained from any lesion using a thin bore needle, smears are prepared and stained to see under the microscope to reach out a diagnosis. This technique carries lesser complications and can be performed in day care. This technique is based on the fact that tumor cells are less cohesive and are easily aspirated. This is used in the diagnosis of breast lumps, thyroid nodules, liver disease, subcutaneous soft tissue mass, salivary gland diseases, and oral diseases.
Martin and Ellis introduced this technique first in the 1930s in the United States, but it never became widespread. Since the 1950s it has been used extensively in Scandinavia and in Holland. Fine needle for aspiration was first introduced in Europe in the 1950’s by Lopez-Cardozo in the Netherlands and Soderstrom in Sweden. Zajicek’s publications from Karolinska Hospital in Stockholm that brought FNAC to international alterations. Since then, it has been extensively used as conventional cytological process to diagnose various pathologies.
The use of liquid-based cytology (LBC) is also gaining interest in the preoperative evaluation of thyroid lesions.[1] The prevalence of thyroid nodules that are palpable is 12.2% worldwide and this number gets increased to 10–14% if detected by any imaging technique.[2,3] The percentage of malignant nodules among thyroid lesions is around 2–7% only, mostly the thyroid nodules are benign.[4] With the use of FNA, the resection of malignant thyroid nodules has been increased from 14% to 50%.[5] Conventional cytological preparations overall have a lot of drawbacks such as dirty and hemorrhagic background which may make the diagnosis difficult. Adequacy is also of concern particularly so when the lesion is hemorrhagic, thus LBC came into existence.[6-9] However, LBC has its own drawbacks and it often removes material which may be of diagnostic significance. It has also been reported that LBC probably changes the morphologic details making it tough to give a diagnosis without adequate exposure to LBC.[10]
Thus, we undertook a pilot study to evaluate the advantages and disadvantages of both the methods of cytology in Indian scenario. This study gives us an idea about the cytomorphological features of various thyroid lesions on conventional cytology and LBC, the comparison between the two methods, and the diagnostic utility of LBC for various ancillary techniques.
MATERIAL AND METHODS
A prospective study had been conducted in the Department of Pathology of Vardhman Mahavir Medical College & Safdarjung Hospital, New Delhi in 2015-2016 on 53 patients where the thyroid swelling was easily visible with the naked eye. In each one, after performing clinical examination like deglutition test, FNA was performed using a 23-gauge needle, 20-mL syringe, and syringe pistol without any USG guidance. In the first step, air-dried smears were made and stained with Giemsa, and alcohol-fixed smears were stained by Papanicolaou stain. Then, whatever material is left in the needle and syringe was transferred into 30 mL of CytoLyt solution (Cytyc) by rinsing the needle and syringe. It was centrifuged for 10 min at 500 g. The supernatant fluid was discarded and the material resuspended in a cytopreservative solution (PreservCyt, Cytyc). After 15 min, the material was processed in BD surepath SOP by standard operative procedure as described by the company. The remaining material was used to make additional smears for immunostaining. Following monoclonal antibodies were used on LBC and conventional cytology as and when indicated;
TTF 1
Thyroglobulin
LCA
Calcitonin
Kapa, Lambda (κ, λ)
T cell markers
B cell markers.
Immunocytochemistry (ICC) method was same as for conventional cytology. Two observers examined the conventional smears and LBCs on different occasions, without knowing the diagnosis. The representative CSs and LBCs were compared for adequacy, cellularity, background blood and cell debris, cell architecture, informative background (such as colloid), presence of cells in monolayer, and nuclear/cytoplasmic details.
Inclusion criteria
All thyroid lesions irrespective of types.
Exclusion criteria
Midline neck swelling that is not arising from thyroid (radiologically proven).
RESULTS
A total of 53 cases were diagnosed by LBC and conventional cytology [Table 1]. The largest number of cases were of colloid nodular goiter amounting to 50.9%. Hashimoto’s/ Lymphocytic thyroiditis which were 26.4% (n = 14). Neoplasms and thyroid hyperplasia were three cases each, i.e. 5.6%. A significant number of cases where no definitive diagnosis could be given were included under descriptive cytology. These were 11.2%.
| S. No. | Cytological diagnosis | No. of cases | Percentage | Cytomorphological findings in Liquid Based Cytology |
|---|---|---|---|---|
| 1. | Colloid nodular goitre | 27 | 50.9 | Colloid globules (small clumps of dense colloid) |
| 2. | Hashimoto’s thyroiditis/lymphocytic thyroiditis | 14 | 26.4 | Lymphoepithelial clusters |
| 3. | Neoplasms | 3 | 5.7 | Nuclear inclusions in Papillary carcinoma |
| 4. | Hyperplasia | 3 | 5.7 | Fire flares |
| 5. | Descriptive | 6 | 11.3 | Better adequacy |
| S. No. | Cytological diagnosis | Morphological features on conventional smears | Morphological features on liquid-based cytology |
|---|---|---|---|
| 1. | Colloid Nodular Goitre | Thyroid follicular cells with colloid in the background Blood in the background [Figure 3] |
Clear background showing only scant colloid in small droplets, no blood in the background [Figure 4] |
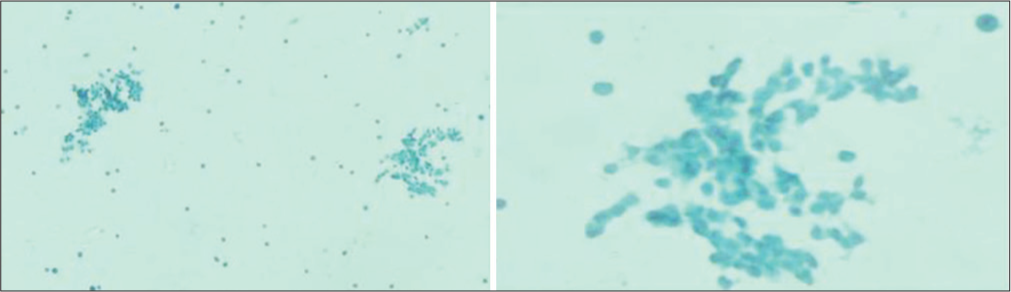
| 2. | Hashimoto’s thyroiditis/lymphocytic thyroiditis | Thyroid follicular cells with lymphocytic impingement. Blood in the background [Figure 1] | Clearer background [Figure 2] |
| 3. | Neoplasms | Cytomorphological features and arrangements easily appreciated on Conventional Smears | Nuclear features are better appreciated on LBC. Easier to perform ancillary techniques like Immunocytochemistry and special stains to reach out a better and early diagnosis [Figures 5 and 6] |

- Conventional cytology preparation showing thyroid follicular cells and lymphocytic impingement and blood in the background.

- Liquid-based cytology preparation showing thyroid follicular cells and lymphocytes with clear background.

- FNA smears show thick colloid against the background of blood.

- LBC smear shows colloid more clearly than the conventional FNA smears.
- Liquid-based cytology preparation showing clearer background and better nuclear morphology of thyroid follicular cells as compared to conventional FNA smears.

- Liquid-based cytology preparations positive for Immunocytochemistry chromogranin in a case of medullary carcinoma thyroid.
DISCUSSION
LBC has gained great success in recent years in gynecological cases. LBC is not only making the diagnosis easier for the pathologist but improving the turnaround time too because of single slide to screen. However, the cellularity in LBC and conventional cytology smears are similar but the nuclear details are clear in LBC.[11] Almost no red blood cells in the background in comparison to the conventional smears where hemorrhagic background hampers the final impression in all the cases.[12,13] In our study, a significant number of our cases (11.2%) were inadequate. However, a repeat slide preparation from the residual material made some of the cases adequate and a proper diagnosis could be made. The easiest lesion to diagnose was the colloid nodular goiter. However, compared to conventional cytology, in LBC colloid appears as small droplets. The morphology of thyroiditis cases was similar in both the methods, though the concentration of lymphocytes appears little more and lymphoepithelial clusters could be identified in LBC.
After making a cytological diagnosis, whatever material remaining in the vial can be used for the application of ancillary techniques such as ICC, flow cytometry, and molecular biology because the LBC method enables the storage of a variable number of cells for up to 6 months after the FNAC.[5,14-17] We have used thyroid markers such as TTF 1, thyroglobulin, LCA, calcitonin which also appeared crisp and clear on LBC. Their visualization being better, helped us in clinching the diagnosis. The number of neoplastic lesions was less in our study, thus a significant comment on morphologic details is not possible. However, it was felt that nuclear groove and inclusions were better appreciated in LBC.[18] Cell Block preparations, a powerful technique, is being used for ages for evaluating tissue morphology and performing immunostaining on sections.[19,20] Cellblock immunohistochemistry is much more reliable owing to the gold standard of histological staining compared to conventional cytology and LBC.[21,22] In a study conducted by Biscotti et al., cell types and cellular arrangements were well preserved in LBC slides. The study also stated that LBC and conventional smears have same diagnostic accuracy.[23] No nuclear and cytoplasmic differences in LBC and conventional smears were noted by another study conducted by Mesonero and Sickel. The diagnostic correlation of both the methods was 90% as per their study.[24] Frost and Cochand-Priollet et al. found variation in nuclear and cytoplasmic features among LBC and CS. Maximum number of cases in their study were turned out to be unsatisfactory.[25,26]
Conventional smears stained with Romanowsky stains or Papanicolaou stain are very well established to diagnose different categories of Bethesda system reporting. A lot of training is required to run both the methods in parallel which may help a reporting cytopathologists in gaining self-confidence and to make them familiar with the distinguishing cytomorphological features of the two methods.
CONCLUSION
LBC is not an alternative to conventional cytology but a good addition to it as it provides excellent nuclear, as well as cytoplasmic details and the drawbacks of conventional cytology such as drying artefact and hemorrhagic background are minimized. It also has an additional advantage of reutilizing the residual material thus preventing a repeat aspiration.
Acknowledgment
I would also like to thank Dr. Sufian Zaheer and Dr. Charanjeet Ahluwalia for their guidance and support which helped me a lot throughout this study. I would also like to thank the staff of the cytopathology section for helping me out with their knowledge and skills.
COMPETING INTERESTS STATEMENT BY ALL AUTHORS
The authors have no conflicts of interest to declare.
AUTHORSHIP STATEMENT BY ALL AUTHORS
Each author has participated sufficiently in the work and takes responsibility for appropriate portions of the content of this article. All authors read and approved the final manuscript.
ETHICS STATEMENT BY ALL AUTHORS
This study was approved by the Institutional Ethics Committee of our institution.
LIST OF ABBREVIATIONS (In alphabetic order)
CS – Conventional Smear
FNAC – Fine needle aspiration cytology
ICC – Immunocytochemistry
LBC – Liquid based cytology
LCA – Leucocyte common antigen
min – Minutes
mL – Milliliter
TTF 1 – Thyroid transcription factor 1.
EDITORIAL/PEER-REVIEW STATEMENT
To ensure the integrity and highest quality of CytoJournal publications, the review process of this manuscript was conducted under a double-blind model (authors are blinded for reviewers and vice versa) through automatic online system.
References
- Fine-needle aspiration cytology of the thyroid: A 12-year experience with 11, 000 biopsies. Clin Lab Med. 1993;13:699-709.
- [CrossRef] [Google Scholar]
- High prevalence of undetected thyroid disorders in an iodine sufficient adult South Indian population. J Indian Med Assoc. 2009;107:72-7.
- [Google Scholar]
- Management of thyroid nodules detected at US: Society of radiologists in ultrasound consensus conference statement. Radiology. 2005;237:794-800.
- [CrossRef] [PubMed] [Google Scholar]
- Screening for cancer with PET and PET/CT: Potential and limitations. J Nucl Med. 2007;48(Suppl 1):4S-18S.
- [Google Scholar]
- Long-term assessment of a multidisciplinary approach to thyroid nodule diagnostic evaluation. Cancer. 2007;111:508-16.
- [CrossRef] [PubMed] [Google Scholar]
- Liquid-based preparations versus conventional cytology: Specimen adequacy and diagnostic assessment in oral lesions. Med Oral Patol Oral Cir Bucal. 2005;10:115-22.
- [Google Scholar]
- Comparison of ThinPrep and conventional preparations on fine needle aspiration cytology material. Acta Cytol. 2000;44:46-50.
- [CrossRef] [PubMed] [Google Scholar]
- Interpretation of fine-needle aspirates processed by the ThinPrep technique: Cytologic artifacts and diagnostic pitfalls. Diagn Cytopathol. 2000;23:6-13.
- [CrossRef] [Google Scholar]
- Comparison of TriPath thin-layer technology with conventional methods on nongynecologic specimens. Acta Cytol. 2000;44:567-75.
- [CrossRef] [PubMed] [Google Scholar]
- How do liquid-based preparations of thyroid fine-needle aspiration compare with conventional smears? An analysis of 5475 specimens. Thyroid. 2015;25:308-13.
- [CrossRef] [PubMed] [Google Scholar]
- Cytomorphological differences between liquid-based cytology and conventional smears in fine-needle aspirates of thyroid lesions. J Cytol. 2018;35:208-11.
- [Google Scholar]
- Utility of a liquid-based, monolayer preparation in the evaluation of thyroid lesions by fine needle aspiration biopsy: Comparison with the conventional smear method. Acta Cytol. 2009;53:130-6.
- [CrossRef] [PubMed] [Google Scholar]
- Split sample comparison of a liquid-based method and conventional smears in thyroid fine needle aspiration. Acta Cytol. 2008;52:313-9.
- [CrossRef] [PubMed] [Google Scholar]
- Techniques for thyroid FNA: A synopsis of the national cancer institute thyroid fine-needle aspiration state of the science conference. Diagn Cytopathol. 2008;36:407-24.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of Thin-Prep and cell block preparation for the evaluation of thyroid epithelial lesions on fine needle aspiration biopsy. Cytojournal. 2008;25:3.
- [CrossRef] [PubMed] [Google Scholar]
- Immunocytochemical evaluation of thyroid neoplasms on thin-layer smears from fine-needle aspiration biopsies. Cancer. 2005;105:87-95.
- [CrossRef] [PubMed] [Google Scholar]
- Changing trends in thyroid practice: Understanding nodular thyroid disease. Endocr Pract. 2004;10:31-9.
- [CrossRef] [PubMed] [Google Scholar]
- Cytological characteristics of papillary thyroid carcinoma on LBC specimens, compared with conventional specimens. Diagn Cytopathol. 2015;43:108-13.
- [CrossRef] [PubMed] [Google Scholar]
- MUC1 and MUC2 expression in pancreatic ductal carcinoma obtained by fine-needle aspiration. Cancer. 2003;99:365-71.
- [CrossRef] [PubMed] [Google Scholar]
- Diagnostic approach to pancreatic tumors with the specimens of endoscopic ultrasound-guided fine needle aspiration. Pathol Int. 2010;60:358-64.
- [CrossRef] [PubMed] [Google Scholar]
- Value of EUS-FNA cytological preparations compared with cell block sections in the diagnosis of pancreatic solid tumours. Cytopathology. 2011;22:174-8.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical utility and diagnostic accuracy of endoscopic ultrasound-guided fine needle aspiration of pancreatic lesions: Saudi Arabian experience. Acta Cytol. 2011;55:26-9.
- [CrossRef] [PubMed] [Google Scholar]
- ThinPrep versus conventional smear cytologic preparations in the analysis of thyroid fine-needle aspiration specimens. Am J Clin Pathol. 1995;104:150-3.
- [CrossRef] [PubMed] [Google Scholar]
- Thyroid fine needle aspiration: A comparison of thin-layer slide preparation with conventional smears. Acta Cytol. 1993;37:795.
- [Google Scholar]
- Utility of thin-layer preparations in thyroid fine-needle aspiration. Cancer Cytopathol. 1998;84:17-25.
- [CrossRef] [Google Scholar]
- Thyroid fine needle aspiration: The morphological features on ThinPrep slide preparations. Eighty cases with histological control. Cytopathology. 2003;14:343-9.
- [CrossRef] [PubMed] [Google Scholar]




