


Translate this page into:
Lymphoproliferative process with reactive follicular cells in thyroid fine-needle aspiration: A few simple but important diagnostic pearls
*Corresponding author
-
Received: ,
Accepted: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 15-year-old female with previous diagnosis at the age of 12 years presented to clinic for follow-up. She complained of dull headaches with mild thyroid enlargement for a period of 1 week. An ultrasound scan revealed a nonenlarging, diffusely heterogeneous thyroid gland with multiple, small, hypoechoic nodules in the isthmus and posteroinferior portion of the left thyroid lobe. She underwent fine-needle aspiration (FNA) biopsies of the nodules in the left thyroid lobe and isthmus. The findings of FNA are shown in Figure 1.
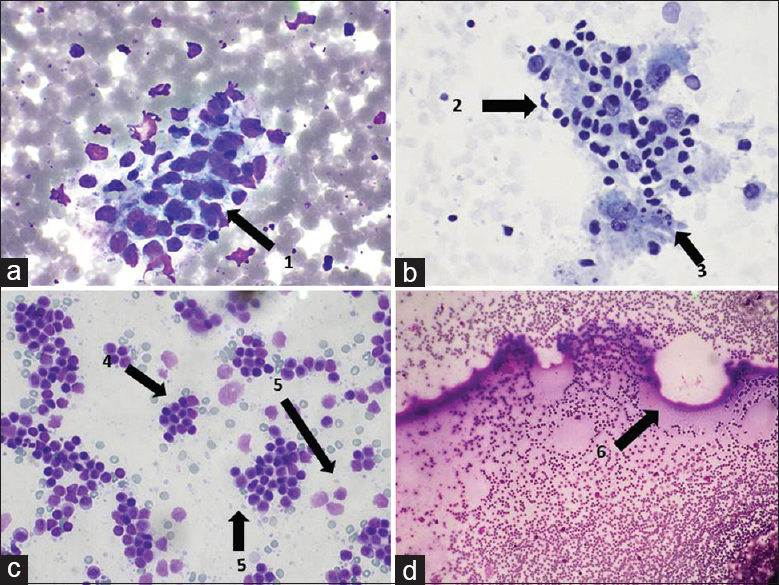
- (a) DQ stain, ×60, (b) PAP stain, ×60, (c) DQ stain, ×60, (d) DQ stain, ×60. (1) Follicular cells with paravacuolar granules. (2) Lymphohistiocytic tangles. (3) Tingible-body macrophages. (4) Predominance of polymorphic lymphocytes. (5) Lymphoglandular bodies in the background. (6) Occasional pass showed some watery colloid
WHAT IS YOUR INTERPRETATION?
-
Papillary thyroid carcinoma (PTC)
-
Hashimoto's thyroiditis
-
High-grade mucosa-associated lymphoid tissue (MALT) lymphoma
-
Follicular neoplasm
Answer: B
Explanation
The aspirates showed abundant polymorphic lymphocytes with lymphohistiocytic tangles showing tingible-body macrophages with relatively scant colloid in the background and with lack of nuclear features of PTC. In addition, the aspirates showed many follicular cells with marked reactive changes as many Hurthle cells with large vesicular nuclei with prominent nucleoli and relatively abundant granular cytoplasm [Figure 2]. Focally, some lymphoepithelial structures with Hurthle cells/thyroid follicular cells infiltrated by lymphocytes were present [Figure 3]. Based on these findings, cytopathologic interpretation of lymphocytic thyroiditis was favored. With reference to the positive serology for antithyroid microsomal antibody, final interpretation was Hashimoto's thyroiditis.
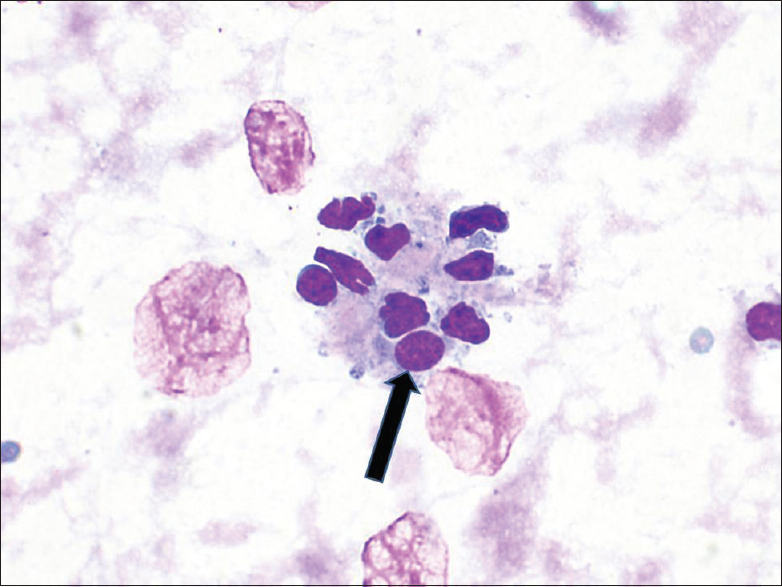
- Arrow depicts Hurthle cells with round nuclei, prominent nucleoli, and granular cytoplasm (DQ stain, × 60)
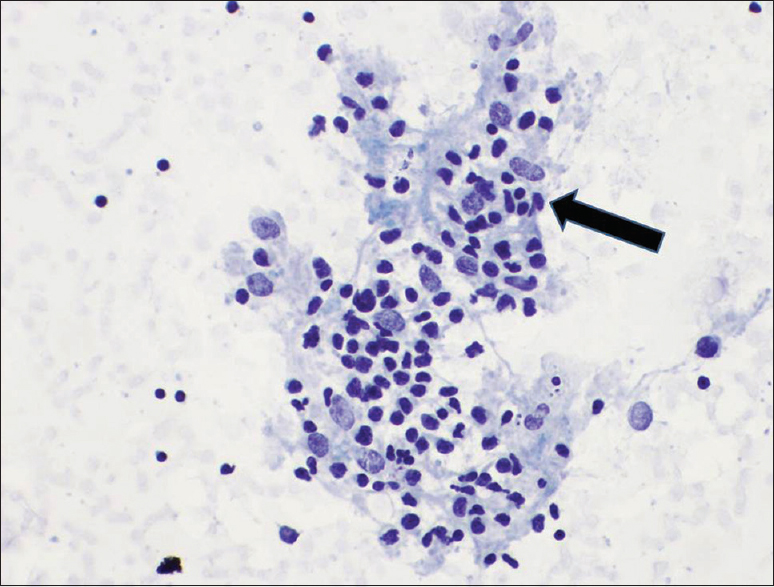
- Arrow depicts lymphoepithelial structures (reactive thyroid follicular cells infiltrated by lymphocytes), pap stain × 60
ADDITIONAL QUIZ QUESTIONS
-
Which combination of methods can best evaluate lymphoma on FNA in setting of Hashimoto's thyroiditis?
-
Wet-fixed Papanicolaou staining with cellblock
-
Wet-fixed May–Grunwald–Giemsa with flow cytometry
-
Air-dried Papanicolaou staining alone
-
Air-dried Wright stain/Diff-Quick stain with flow cytometry
-
Answer: D
Explanation
The characteristic cytomorphological features of lymphocytes [Figure 1] and other features including lymphoglandular bodies [Figure 1c] in lymphoproliferative processes are best appreciated in air-dried Romanowsky stain, like Wright stain/Diff-Quick stain. Flow cytometry immunocharacterizes the lymphoid population as reactive process versus lymphoma with subtyping.
2. A cellular aspirate predominantly shows cells with abundant, fine granular cytoplasm, large, central, or eccentrically placed round nuclei with prominent nucleoli, and varying nuclear sizes. The cells are present as crowded groups with syncytial arrangement and have little to no colloid and/or lymphocytes in the background. Which of the following is the most likely cytopathologic interpretation?
-
Lymphocytic thyroiditis
-
Follicular neoplasm, Hurthle cell type
-
Multinodular goiter
-
Hashimoto's thyroiditis
Answer: B
Explanation
Hurthle cell neoplasms (oncocytic variant of follicular neoplasm) have >75% of follicular cells as oncocytes (Hurthle cells) with round nuclei showing prominent nucleoli, and abundant eosinophilic, granular cytoplasm, and without a significant amount of colloid. Compared to lymphocytic thyroiditis/Hashimoto's thyroiditis, the number of lymphocytes in the background is insignificant, if any. The aspirates from lymphocytic thyroiditis/Hashimoto's thyroiditis may show significant number of lymphoepithelial structures with lymphocytes infiltrating and destroying Hurthle cells. If the aspirate is an oncocytic variant of PTC, nuclear features of PTC would be evident.
3. As opposed to classic Hashimoto's thyroiditis, Juvenile Hashimoto's thyroiditis?
-
May undergo remission
-
Will rapidly progress to atrophy and fibrosis
-
Will present with follicular epithelial cells surrounded by lymphocytes on FNA
-
Will have goiter
Answer: A
Explanation
The most common cause of hypothyroidism in children and adolescents is Hashimoto's thyroiditis and it may undergo remission.
REVIEW OF TOPIC
Hashimoto's thyroiditis is also known as struma lymphomatosa, lymphocytic thyroiditis, or chronic autoimmune thyroiditis. It is characterized by autoimmune destruction of the thyroid gland and is the most common cause of hypothyroidism in iodine-sufficient regions. It is more common in females than males. It is classically seen in the fifth decade; however, a juvenile form exists that presents at a mean age of 11 years.[1]
In symptomatic patients, the initial presentation may be that of hyperthyroidism as a result of the destruction of follicles. The destruction of the thyroid gland progresses to hypothyroidism, with decreased T4 and increased thyroid-stimulating hormone. Diffuse enlargement of the thyroid may occur at presentation, though less commonly it can present as one or more nodules. Autoantibodies such as antithyroglobulin and antithyroid peroxidase may also be present and relate to thyroid damage. Most patients have detectable serum concentrations of antibodies against at least one thyroid antigen.
Pathogenesis is thought to include genetic and environmental factors leading to CD4+ T-cell sensitization to thyroid antigens. CD8+ T-cells, cytokines, and antibody-dependent cell-mediated cytotoxicity are all thought to play a role in the destruction of the gland.[2]
Typical findings on histology include Hurthle cells, which are reactive, polyclonal thyroid follicular cells with eosinophilic granular cytoplasm and nuclei with prominent nucleoli.[1] Also present is variable proportion of chronic inflammation including lymphoid aggregates with and without germinal centers. Both B- and T-cells infiltrate the thyroid gland. Plasma cells may also be seen. Fibrosis and atrophy of the gland may become more prominent later in the course of the disease.
Hashimoto's thyroiditis confers an increased risk for MALT lymphoma (extranodal marginal zone B-cell lymphoma) (estimated up to 23.5%).[3] This may present clinically as an enlarged gland. Moreover, clinical literature recognizes a significant association between the prevalence of PTC and Hashimoto's thyroiditis (24%–26.6% PTC found in thyroidectomies).[45] These cases were mostly younger women with relatively less aggressive PTC which did not metastasize to lymph nodes. Long-term follow-up of patients is important for surveillance of neoplastic complications. FNA is a minimally invasive modality for evaluation of thyroid nodules in this setting to rule out neoplastic processes.
FNA of the thyroid is considered superior to antibody screening alone and carries a 92% diagnostic accuracy.[36] FNA can be used for surveillance of neoplastic complications in elderly patients with long-standing Hashimoto's thyroiditis.[6] Aspirates with predominance of oncocytic follicular epithelial cells with many lymphocytes [Figure 1] distinguish Hashimoto's thyroiditis from neoplasms.[7] The lymphocytes aspirated directly from the pathology usually show crowding with tendency for crushing artifact with DNA strands while spreading the smears between two glass slides, distinguishing such lymphocytes from lymphocytes associated with chronic inflammation in multinodular thyroid. Lymphocytes from chronic inflammatory infiltrates show relatively spared polyhedral shape with scattered single cells randomly sprinkled in the background.
Cytopathologic interpretation of Hashimoto's thyroiditis is made as lymphocytic thyroiditis by an FNA smear consisting of Hurthle cells [Figure 2], polymorphic population of lymphocytes with lymphoglandular bodies [Figure 1c], lymphohistiocytic tangles as collection of lymphocytes and histiocytes with tingible-body macrophages [Figure 1b], and lymphocytic infiltration of follicular cells (lymphoepithelial structures) [Figure 3] without colloid or with minimal watery colloid [Figure 1d].[38]
The differential diagnosis is broad based on cytopathological findings. The first differential is Hurthle cell neoplasm which is characterized by relatively cellular aspirates with numerous three-dimensional groups of oncocytic follicular cells without significant number of lymphocytes. Nodular goiter with prominent oncocytic changes should also be ruled out. Here, sheets/monolayers of thyroid follicular cells arranged in honey-combs are admixed with reactive Hurthle cells present as repair-like groups with school of fish pattern, with significant proportion of colloid in the background.[9] However, a few scattered lymphocytes may be present as part of focal chronic inflammation in multinodular thyroid. Medullary carcinoma with Hurthle cell-like oncocytic changes may sometimes be confusing, but immunoreactivity for calcitonin, carcinoembryonic antigen, with nonimmunoreactivity for thyroglobulin with elevated calcitonin blood level would favor medullary carcinoma. A rare possibility is carcinoma with thymus-like elements which shows three-dimensional clusters with occasional lymphocytes. Individual keratinization and orangeophilic cytoplasm may be seen. Lastly, PTC with oncocytic (Hurthle cell) changes should be excluded in oncocytic thyroid neoplasms that show nuclear features of PTC such as ground glass nuclei, intranuclear inclusions and longitudinal nuclear grooves.
SUMMARY
FNA is a minimally invasive surveillance for potential neoplasms arising in the setting of Hashimoto's thyroiditis. Onsite adequacy evaluation with elective flow cytometry is an excellent tool for ruling in/ruling out a lymphoproliferative process, especially low-grade MALT lymphoma. When FNA yields an aspirate with predominance of lymphocytes, ancillary tests should be performed to rule out low-grade MALT lymphoma. Predominance of Hurthle cells in three-dimensional solid groups, trabecular pattern, or other epithelial structures without significant number of lymphocytes and without significant colloid in the background would favor Hurthle cell neoplasm or oncocytic variants of other thyroid neoplasms. Relevant features should be properly scrutinized and considered. Potential pitfalls include missing oncocytic variants of various neoplasms including PTC (intranuclear pseudoinclusions/nuclear grooves with nuclear irregularity), and medullary carcinoma (calcitonin immunoreactivity/elevated blood calcitonin level).
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
COMPETING INTERESTS STATEMENT BY ALL AUTHORS
The author(s) declare that they have no competing interests.
AUTHORSHIP STATEMENT BY ALL AUTHORS
All authors of this article declare that we qualify for authorship as defined by ICMJE http://www.icmje.org/#author.
Each author has participated sufficiently in the work and takes public responsibility for appropriate portions of the content of this article.
OS helped draft the manuscript and prepared the images.
BB, LH and YL helped draft the manuscript.
VS helped with editing, revising and drafting of the manuscript.
Each author acknowledges that this final version was read and approved.
ETHICS STATEMENT BY ALL AUTHORS
As this is Quiz Case without identifiers, our institution does not require approval from the Institutional Review Board (or its equivalent).
LIST OF ABBREVIATIONS (In alphabetic order)
FNA - Fine needle aspiration
PTC - Papilary thyroid carcinoma
MALT - Mucosa-associated lymphoid tissue
EDITORIAL/PEER-REVIEW STATEMENT
To ensure the integrity and highest quality of CytoJournal publications, the review process of this manuscript was conducted under a double-blind model (the authors are blinded for reviewers and vice versa) through automatic online system.
REFERENCES
- Hashimoto thyroiditis: Clinical and diagnostic criteria. Autoimmun Rev. 2014;13:391-7.
- [Google Scholar]
- Cytomorphologic spectrum of lymphocytic thyroiditis and correlation between cytological grading and biochemical parameters. J Cytol. 2016;33:145-9.
- [Google Scholar]
- Fine needle aspiration cytology of Hashimoto's thyroiditis – A diagnostic pitfall with review of literature. J Cytol. 2011;28:210-3.
- [Google Scholar]
- Coexistence of papillary thyroid cancer with Hashimoto thyroiditis. Langenbecks Arch Surg. 2013;398:389-94.
- [Google Scholar]
- Hashimoto's thyroiditis: Celebrating the centennial through the lens of the Johns Hopkins hospital surgical pathology records. Thyroid. 2013;23:142-50.
- [Google Scholar]
- Cytological diagnosis of thyroid nodules in Hashimoto thyroiditis in elderly patients. BMC Surg. 2013;13(Suppl 2):S41.
- [Google Scholar]
- The Bethesda System for Reporting Thyroid Cytopathology: Definitions, Criteria, and Explanatory Notes. New York: Springer; 2017.
- Common Diagnostic Pitfalls in Thyroid Cytopathology. Switzerland: Springer; 2016.




