


Translate this page into:
Primary ovarian non-Hodgkin lymphoma: Diagnosis of two cases on fine needle aspiration cytology
*Corresponding author
-
Received: ,
Accepted: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Lymphoma of the female genital tract is a rare condition. Involvement of the ovary by non- Hodgkin lymphoma (NHL) is usually secondary to systemic disease and primary ovarian lymphomas are unusual. In most cases, the diagnosis is not suspected initially and is confirmed only after detailed histopathological evaluation. We describe two cases of primary ovarian NHL which were diagnosed on fine needle aspiration cytology (FNAC). One of the patients was a 40 years old female who presented with abdominal distension and lump. She was found to have bilateral adnexal masses on ultrasound and computed tomography (CT) scan. A USG guided fine needle aspiration of the ovarian masses was performed, following which a diagnosis of primary ovarian diffuse large B-cell lymphoma was established. The second patient was a 14 years old female who presented with pelvic lump, which was lobulated and mildly enhancing on contrast enhanced CT. A diagnosis of high grade NHL of ovaries was made on cytology. Subsequently, the lymphoma was characterized as Burkitt's on histopathological examination. Both the patients were started on R-CHOP chemotherapy regimen. FNAC serves as an extremely useful minimally invasive procedure for the diagnosis of ovarian lymphomas and early institution of appropriate chemotherapeutic regimens.
Keywords
Non-Hodgkin lymphoma
ovarian
ultrasound guided fine needle aspiration

INTRODUCTION
Non-Hodgkin lymphoma (NHL) may involve the gynecologic tract. Ovarian involvement by NHL is usually secondary, occurring as a part of the systemic disease. Localized, presumably primary, NHL of the ovary is rare.[123] We present two cases of primary ovarian lymphoma (POL) which were diagnosed on ultrasound guided fine needle aspiration cytology. To the best of our knowledge, diagnosis of ovarian lymphoma on cytology has only sparsely been described in a few series on fine needle biopsies of ovarian tumors and not discussed primarily in detail in the literature.
CASE REPORTS
Case 1
A 40-year-old female presented to the gynecology outpatient department with the complaints of abdominal distension and lump for 1-month. The hematological and biochemical parameters were all within the normal limits. USG abdomen revealed bilateral homogenous adnexal masses. Computed tomography (CT) scan of abdomen showed bilateral large heterogenously enhancing adnexal masses measuring approximately 10 cm × 7 cm (right) and 9 cm × 6 cm (left) with discrete retroperitoneal lymph nodes (varying in maximum dimension from 1.5 to 2.5 cm) compressing both the ureters resulting in hydronephrosis of both the kidneys [Figure 1]. An impression of malignant ovarian masses was suggested radiologically. The patient was planned for ultrasound guided fine needle aspiration (FNA). Aspiration cytology smears from bilateral ovarian masses were highly cellular and showed predominantly dispersed monomorphic population of lymphoid cells [Figure 2]. The lymphoid cells were large sized with minimal amount of cytoplasm and conspicuous nucleoli. On immunocytochemistry, the lymphoid cells were positive for CD 20 and negative for CD 3. Thus, a diagnosis of NHL of B-cell immunophenotype involving both the ovaries was made. Biopsy of the adnexal mass was also performed. The histopathological examination confirmed the diagnosis of NHL, diffuse large B-cell lymphoma (DLBCL) type. The patient was evaluated for the presence of hematological involvement by peripheral blood and bone marrow examination and lymph node involvement by physical examination and imaging, but was found negative for both. Only the retroperitoneal lymph nodes were enlarged which showed features of reactive hyperplasia on FNA. Hence, a diagnosis of primary bilateral ovarian lymphoma was considered and the patient was started on chemotherapy regimen including rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisolone (R-CHOP). The patient is in remission since 7 months.

- Computed tomography of abdomen showing bilateral large adnexal masses with bilateral hydronephrosis due to compression of ureters
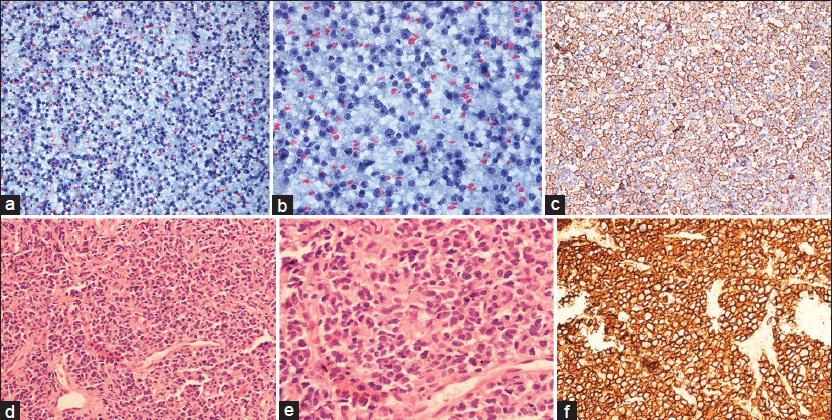
- (a) Dyscohesive tumor cells, Pap, ×200; (b) the tumor cells have large round pleomorphic nuclei and conspicuous nucleoli. Lymphoglandular bodies are also seen in the background, Pap, ×400; (c) tumor cells show immunopositivity for CD20 × 200; (d) tumor cells dispersed singly, H and E, ×100; (e) the tumor cells are large, pleomorphic and show mitoses, H and E; (f) strong immunopositivity for CD20 is seen in the tumor cells, ×200
Case 2
A 14-year-old female presented to the surgical outpatient department with the complaint of pelvic lump since 1-month. Contrast enhanced CT showed a well-defined lobulated mildly enhancing soft tissue pelvic mass measuring 12 cm × 10 cm with no separate and clear delineation of ovaries. Bilateral hydronephrosis was also evident. Subsequently, USG guided FNA was performed. Cytology smears showed a predominantly dispersed population of large cells with scant cytoplasm and conspicuous nucleoli [Figure 3]. A diagnosis of poorly differentiated malignant tumor possibly high grade NHL was suggested. Immunocytochemistry could not be carried out due to lack of adequate material. The patient underwent exploratory laparotomy, and bilateral ovarian masses were resected. The histopathological examination showed complete replacement of ovarian parenchyma by intermediate sized lymphoid cells with brisk mitoses and apoptosis. The lymphoid cells were immunopositive for CD 20 and BCL 6 but negative for BCL 2, CD 10, CD 34, and CD 3. MIB 1 labeling index was approximately 98%. Thus, a final diagnosis of Burkitt's lymphoma was made on the basis of morphological features and immunohistochemical results. BCL 2 negativity helped in excluding DLBCL in addition to the morphological features. No evidence of hematological (peripheral blood and bone marrow examination) and lymph node involvement was found, even after an elaborate clinical and radiological workup. The patient was started on systemic chemotherapy and is in remission since 3 months.
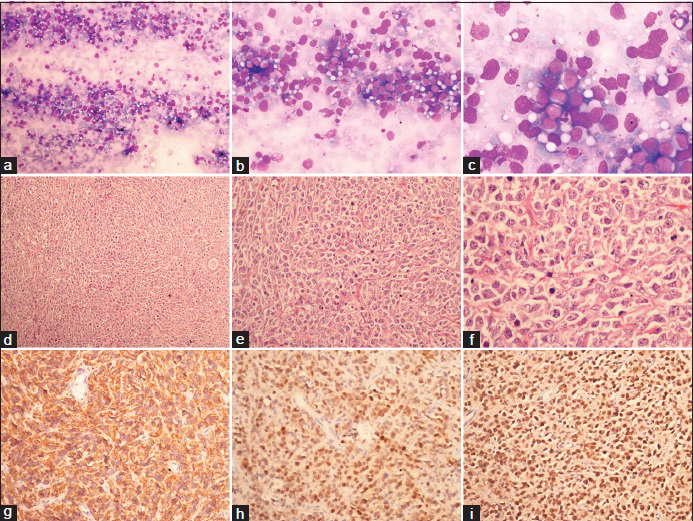
- (a) Predominantly dispersed tumor cells; MGG, ×100; (b) high nucleocytoplasmic ratio and moderate pleomorphism; MGG × 200; (c) minimal vacoulated cytoplasm, opened up nuclear chromatin and small nucleoli at places; MGG × 400; (d) tumor cells arranged in solid sheet and focally in cords; H and E, ×100; (e) minimal cytoplasm, pleomorphic nuclei and frequent apoptoses; H and E, ×200; (f) small nucleoli. Macrophages with engulfed debris are also seen; H and E, ×400; (g) tumor cells are immunopositive for CD20 (h) BCL6; (i) MIB1 labeling index of 98% ×200
DISCUSSION
Involvement of the ovary by malignant lymphoma can be primary or secondary.[123] POL is extremely rare accounting for 0.5% of all NHL and 1.5% of all ovarian neoplasms.[4] Lymphomas of the ovary may occur at any age, but mostly women in their 40s are affected. Whether primary or secondary, ovarian lymphomas may have a varied presentation, most of them being discovered incidentally during the work up for pelvic or abdominal complaints.[12356]
Histologically, the normal ovary is devoid of any lymph tissue; therefore, the occurrence of lymphomas primarily arising in the ovaries has long been debated.[7] Benign lymphoid aggregates seen in the ovarian hilum and the chronic inflammatory cells found in the ovaries in response to pelvic inflammatory diseases have been suggested as the possible origins of POL.[68] The most common types of NHL encountered in the ovary are a diffuse large cell, Burkitt's, and follicular lymphoma.[2]
Fox et al., described the diagnostic criteria for POL as: (a) A disease confined to ovary, (b) the absence of disease in blood and bone marrow; (c) the extra ovarian deposits if any should appear at least after 6 months. With the above mentioned criteria, the diagnosis of POL becomes rare.[9] Our cases fulfilled the criteria. Ferrozzi et al. described the radiological findings in NHL of the ovaries. The Magnetic resonance imaging findings included solid bilateral masses, which were low signal intensity on T1-weighted images and mildly high signal intensity on T2-weighted images.[10] CT scan showed hypodense lesions with mild contrast enhancement, whereas ultrasonographic findings were nonspecific with hypoechoic patterns.[7]
Malignant lymphoma of the ovary may be confused with other primary ovarian tumors such as dysgerminoma, granulocytic sarcoma, granulosa cell tumor, and undifferentiated carcinoma.[15] On cytological examination, features such as singly dispersed cell population and monomorphic looking cells along with lymphoglandular bodies in an aspirate from ovarian masses, especially bilateral, with suspicious features on radiology warrants an inclusion of NHL in the differentials. Immunocytochemical evaluation helps in excluding the differentials. Dysgerminoma shows immunopositivity for placental alkaline phosphatase and CD 117 whereas granulosa cell tumor cells are immunopositive for inhibin and calretinin. Poorly differentiated and undifferentiated carcinoma can be excluded by negative cytokeratin and epithelial membrane antigen staining. Negative staining for myeloperoxidase helps in ruling out the possibility of granulocytic sarcoma.
Flow cytometry is increasingly being used as a technique for determination of surface antigens on cells teased from masses with suspected lymphoma. FNA combined with flow cytometry obviates the need for a surgical biopsy. Loss of architectural relationships during processing of specimens for flow cytometry is a major problem when small foci of lymphoma or tumor cells exist together with large amounts of stroma or normal lymphocytes.[11] Fluorescent in situ hybridization (FISH) can be used to detect numerical and structural chromosomal abnormalities. Interphase and fiber FISH can be used on cytology samples. Cytomorphological evaluation and immunocytochemistry are followed by flow cytometry and FISH to obtain exact subclassification and prognostication.[12]
Lymphomas of the ovary should be treated with systemic chemotherapy, even if the spread beyond the ovary is not detected by the staging procedure.[4] Primary extra nodal lymphoma runs a less aggressive course with 5 years survival rate of 80% as compared to secondary malignant lymphoma, which has a 5 years survival rate of only 33%.[35] Prognostic factors include the clinical stage, mode of onset, histologic type, and phenotype.[4]
This case series highlights the importance of preoperative rapid cytological diagnosis of ovarian lymphoma by use of USG guided FNA in conjunction with immunocytochemistry. Moreover, subtle clinical and radiological unusual findings should be carefully looked for suspecting such a diagnosis preoperatively.
COMPETING INTERESTS STATEMENT BY ALL AUTHORS
The authors declare that they do not have competing interests.
AUTHORSHIP STATEMENT BY ALL AUTHORS
All authors declare that they qualify for authorship as defined by ICJME.
ETHICS STATEMENT BY ALL AUTHORS
No experimental research has been carried out with regard to the manuscript.
LIST OF ABBREVIATIONS (In alphabetic order)
CT - Computed Tomography
DLBCL - Diffuse Large B-Cell Lymphoma
FISH - Fluorescent in situ hybridization
FNA - Fine Needle Aspiration.
FNAC - Fine Needle Aspiration Cytology
NHL - Non-Hodgkin Lymphoma
POL - Primary Ovarian Lymphoma.
EDITORIAL/PEER-REVIEW STATEMENT
To ensure the integrity and highest quality of CytoJournal publications, the review process of this manuscript was conducted under a double-blind model (authors are blinded for reviewers and vice versa) through automatic online system.
REFERENCES
- Lymphomas or leukemia presenting as ovarian tumors. An analysis of 42 cases. Cancer. 1983;52:1933-43.
- [Google Scholar]
- Ovarian non-Hodgkin's lymphoma: A clinicopathologic study of eight primary cases. Mod Pathol. 2001;14:1093-9.
- [Google Scholar]
- Ovarian metastases of lymphomas and other haematological malignancies. CME J Gynecol Oncol. 2004;9:195-7.
- [Google Scholar]
- Primary bilateral non hodgkin's ovarian lymphoma – A case report. JKIMSU. 2012;1:155-9.
- [Google Scholar]
- Malignant lymphomas involving the ovary. A clinicopathologic analysis of 39 cases. Am J Surg Pathol. 1993;17:154-70.
- [Google Scholar]
- Primary non-Hodgkin's lymphoma of the ovaries: Imaging findings. Br J Radiol. 2007;80:e155-8.
- [Google Scholar]
- Primary precursor B-cell lymphoblastic lymphoma of the ovary: Case report and review of the literature. Int J Gynecol Pathol. 2008;27:412-7.
- [Google Scholar]
- Malignant lymphoma presenting as an ovarian tumour: A clinicopathological analysis of 34 cases. Br J Obstet Gynaecol. 1988;95:386-90.
- [Google Scholar]
- Ovarian lymphoma. Findings with ultrasonography, computerized tomography and magnetic resonance. Radiol Med. 1998;95:493-7.
- [Google Scholar]
- The role of flow cytometry in the diagnosis of lymphoma: A critical analysis. Ann Clin Lab Sci. 1994;24:6-11.
- [Google Scholar]
- Best Practice No 185. Cytological and molecular diagnosis of lymphoma. J Clin Pathol. 2005;58:561-7.
- [Google Scholar]




