


Translate this page into:
Squash surprise in an elderly female


-
Received: ,
Accepted: ,
How to cite this article: Gupta S, Singh S, Kumari N, Rajwanshi A. Squash surprise in an elderly female. 2024;21:18. doi: 10.25259/ Cytojournal_94_2023
QUIZ DESCRIPTION
A 57-year-old female presented with nausea, vomiting, and headache over a year. The patient had no specific complaints except for gradual weight loss over the past year. Computed tomography scan (CT) was done. T2-weighted sagittal images show an ill-defined T2 hyperintense cystic space occupying a lesion in the occipital lobe. There is ipsilateral compression of the occipital horn of the ventricle and disproportionate perilesional edema with midline shift [Figure 1a]. A craniotomy was performed on the suspicion of a glioma. Intraoperatively, the tumor was yellowish white non-vascular, and soft surrounded by viscous yellow fluid. The bits of tumor tissue sent for squash diagnosis were yellow, firm, and difficult to squash and spread. Rapid hematoxylin and eosin stain was performed.
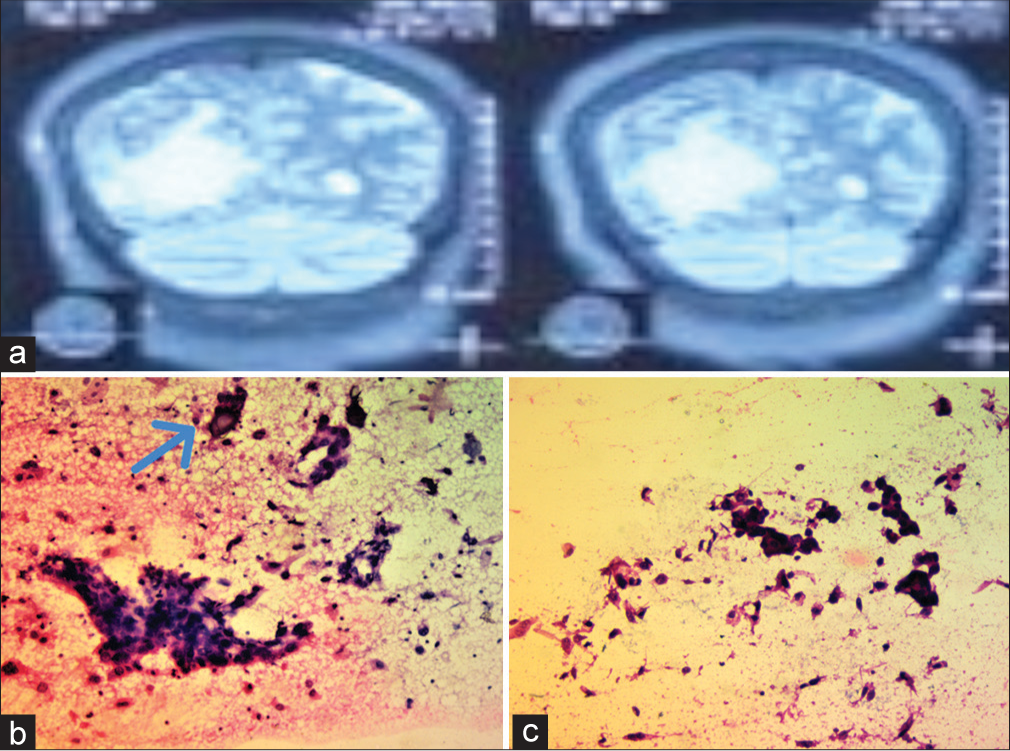
- (a) Computed tomography (CT) image showing ill defined T2 hyperintense cystic space occupying lesion in the occipital lobe. (b-c) Squash cytology smears showing cohesive clusters of hyperchromatic tumor cells against a thin mucoidy background and foci of calcification(blue arrow). (b, c: Hematoxylin and Eosin H&E, 200x and 40x.).
Definitive sections were sent for histopathology and immunohistochemical staining was done.
MORPHOLOGY QUIZ
-
What is the diagnosis based on the clinical history, imaging findings, and photomicrographs [Figure 1] provided?
Glioma
Meningioma
Metastatic carcinoma
Lymphoma
-
Which of the following immunohistochemical panels would be most useful for diagnosis?
CK7, CK20, TTF-1, GATA3, PAX-8, CDX2
CK7, CK20, Calretinin, WT1
IDH1/2, ATRX, P53
GFAP, Vimentin, NeuN
Answers
1. (c) Metastatic carcinoma
2. (a) CK7, CK20, TTF-1, GATA3, PAX-8, and CDX2
EXPLANATION
Squash smear cytology is a rapid and reliable method for intraoperative diagnosis of inflammatory and neoplastic brain lesions.[1]
Squash smears were moderately cellular and showed cohesive clusters and glandular arrangement of tumor cells against a thin mucoid background [Figure 1b-c]. The tumor cells had round to oval hyperchromatic nuclei and a moderate amount of cytoplasm. A focus shows calcification. The findings were suggestive of a non-glial lesion, possibly metastases. Histopathology sections showed well-formed glands and sheets of tumor cells with pools of mucin and psammoma bodies confirming the diagnosis of metastatic adenocarcinoma [Figure 2a-d].
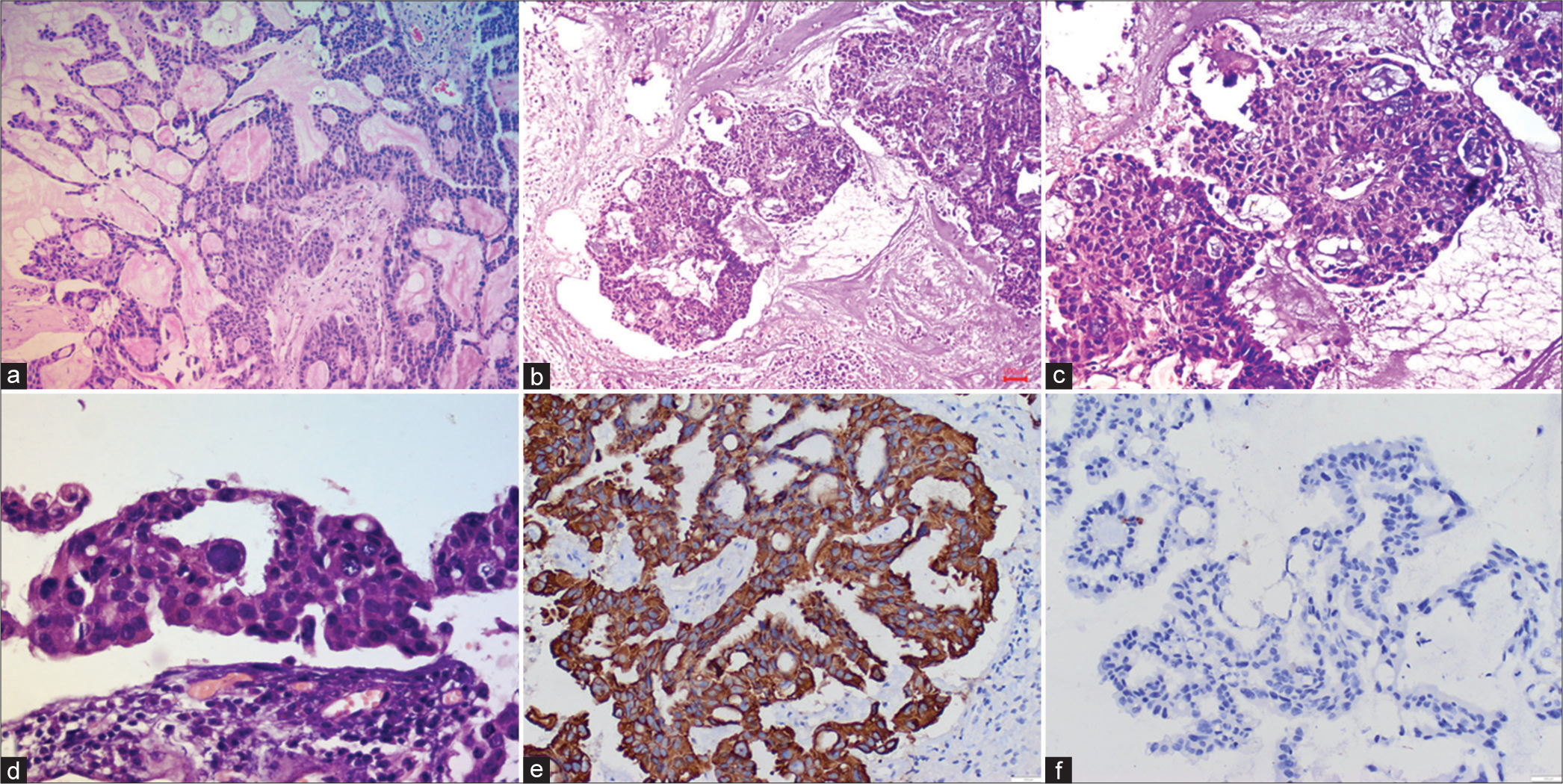
- Microphotograph panel (a-d) showing well-formed glands and solid sheets of tumor cells with pools of mucin and focal calcification (hematoxylin and eosin stain) (a: 40x, b: 100x, c: 200x, d: 400x), (e) Tumor sections showing immunopositivity for CK7 200x (f) Tumor sections showing immunopositivity for CK20 [IPOX] 200x.
The most common tumors leading to brain metastases include lung and breast followed by renal tumors. In the present case, the tumor cells showed strong immunopositivity for CK7 and were immunonegative for CK20 [Figure 2e and f]. In a female patient, CK7-positive and CK20-negative adenocarcinomas warrant the search for primary in the lung, breast followed by the uterus (endometrial), pancreas, and gallbladder.
ADDITIONAL QUIZ QUESTIONS
3. Which of the following is the most common intracranial tumor?
Gliomas
Metastases
Meningioma
Lymphoma
4. Which of the following is a differential diagnosis of metastases to the brain?
Abscess
Parasitic infestation
Primary tumor-glioma/ependymoma
All of the above
Answers
3. (b) Metastas es
4. (d) All of the above
EXPLANATION
The differential diagnosis of metastases to the brain includes primary tumors of the brain, parasites, and abscesses.
Squash cytology smears of glial tumors are cellular with specific cytomorphological features of the tumor cells. For instance, the squash smears of low-grade gliomas show sparse cellularity of tumor cells in a fibrillary background in contrast to high-grade gliomas which are characterized by hypercellularity, endothelial proliferation, necrosis, and mitoses. Necrosis is also often noted in cases of brain abscess, characteristically described as liquefactive necrosis. Fungal, tubercular, and parasitic infestation can also show necrotic background.
BRIEF REVIEW OF TOPIC
Metastases to the brain are a known complication in approximately 20% of malignancies.[2] Brain metastases are often detected in CT and magnetic resonance imaging scans and previously known cases of malignancy during routine investigations. In most cases, metastases travel through the hematogenous route from lung tumors, breast carcinomas, renal cell carcinomas, and melanomas by breaching the blood–brain barrier.[3] Metastases are usually noted as intra-axial, intraparenchymal masses with a varied range of radiological differential diagnoses including gliomas, abscesses, and infections. Furthermore, in approximately 15% of cases, a primary tumor is not found.[4] In the index case, in the absence of any specific complaints elsewhere and a mass lesion in the brain, the suspicion of metastases was unlikely on clinical and radiological examination.
These cases are challenging and the surgeon relies on intraoperative diagnosis for immediate surgical management. In such scenarios, squash cytology can be reliably used to differentiate between metastatic from primary central nervous system neoplasms.
The squash smear cytomorphology depends on the type of primary tumor (adenocarcinoma, small cell carcinomas, melanoma, lymphoma, etc.). An algorithmic approach and workup with immunohistochemical markers can be useful for the detection of the primary tumor.
Immunohistochemical panel for morphologically designated adenocarcinoma of unknown primary involves the cytokeratin status (CK7 and CK20). Further organ-specific markers can be tested after analysis of CK7 and CK20 expression.[5]
In the index case, CK7 immunopositivity was found; however, the patient was lost to follow-up and further markers were not done.
Extensive radiological examination and accurate subtyping of the primary tumor enable the pathologist to choose the apt immunohistochemistry marker panel and document the origin of the tumor.
SUMMARY
The awareness of metastatic carcinoma as a differential diagnosis on cytology and identification of cytomorphological features can guide the surgeon and management of the patient.
ABBREVIATIONS
CT - Computed topography
CK – Cytokeratin
IPOX – Immunoperoxidase
AUTHOR CONTRIBUTIONS
SG: Involved in diagnosis, conceptualization, drafting, and editing the manuscript. SS: Involved in patient management and editing the manuscript. NK: Involved in diagnosis and editing the manuscript. AR: Involved in reviewing and editing the manuscript. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
ETHICAL APPROVAL
This study was approved by the Institutional Ethics Committee AIIMS Raebareli, (approval no. 2024 -5 - OTHEXP- 7).
Written informed consent was obtained from all the participants.
CONFLICT OF INTEREST
Given his role in the International Editorial panel, Arvind Rajwanshi had no involvement in the peer-review of this article and has no access to information regarding its peer review. The authors declare no conflict of interest.
EDITORIAL/PEER REVIEW STATEMENT
To ensure the integrity and highest quality of Cytojournal publications, the review process of this manuscript was conducted under a double-blind model (authors are blinded for reviewers and vice versa) through an automatic online system.
FUNDING
Not applicable.
References
- Intraoperative squash cytology: accuracy and impact on immediate surgical management of central nervous system tumors: Impact of squash cytology on immediate surgical management. Cytopathology. 2012;23:308-14.
- [CrossRef] [PubMed] [Google Scholar]
- Epidemiology of brain metastases. Neurosurg Clin N Am. 2020;31:481-8.
- [CrossRef] [PubMed] [Google Scholar]
- Metabolism in the progression and metastasis of brain tumors. Cancer Lett. 2022;539:215713.
- [CrossRef] [PubMed] [Google Scholar]
- Brain metastasis from unknown primary tumour: Moving from old retrospective studies to clinical trials on targeted agents. Cancers (Basel). 2020;12:3350.
- [CrossRef] [PubMed] [Google Scholar]




