


Translate this page into:
A case of large cell neuroendocrine carcinoma of the uterine cervix misdiagnosed as adenocarcinoma in Thinprep cytology test
*Corresponding author
-
Received: ,
Accepted: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Large cell neuroendocrine carcinoma (LCNEC) of uterine cervix is a rare malignancy with aggressive behavior and poor clinical outcome even in its early stage. Few cytopathologic features of cervical LCNEC have been reported previously. A 57-year-old postmenopausal African American female, presented to the local health department with a chief complaint of heavy vaginal bleeding. A 45-year-old female presented with 20 months of vaginal pruritus and foul odor. Cervical malignancy was suspected by pelvis magnetic resonance imaging. Thinprep cytology test demonstrated ball-like tumor cell clusters in a necrotic background. Cytologic diagnosis of adenocarcinoma was rendered. However, the histologic and immunohistochemical examination of cervical biopsy revealed the LCNEC of the uterine cervix. Due to its rarity, LCNEC may pose a diagnostic challenge in cervical cytology. Cytopathologists should pay attention to the cytological features of cervical LCNEC, such as rosettoid pattern, nuclear molding, and thin nuclear membrane for differentiation from other mimics.
Keywords
Carcinoma
cervix uteri
cytology
neuroendocrine

INTRODUCTION
Large cell neuroendocrine carcinoma (LCNEC) of uterine cervix is a rare malignancy with aggressive behavior and poor prognosis even in its early stage.[1] Thus, recognizing the entity of LCNEC on cervical Papanicolau (PAP) smear is very important to improve its clinical outcome. The histopathologic features of cervical LCNEC are well-defined.[12] However, few cases of cytologic findings have been reported.[2345] Recently, we experienced a case of cervical LCNEC in Thinprep cytology test. We describe a case of LCNEC of the cervix, with a focus on its cytologic features.
CASE REPORT
A 45-year-old female presented with 20 months of vaginal pruritus and foul odor. The patient had a history of anti-inflammatory treatment at local health department. She was referred to tertiary care center for further evaluation and treatment. Colposcopic examination showed an irregular surface and bleeding of cervix, which was suspected the high grade squamous intraepithelial lesion. Pelvis magnetic resonance imaging revealed cervical malignancy with stage IB1. The obtained cervical smear sample was processed using a liquid based ThinPrep technique. The cytologic features showed many ball-like tumor cell clusters in a necrotic background [Figure 1a]. These large neoplastic cells showed moderate amount of cytoplasm, prominent nucleoli, and nuclear overlapping [Figure 1b]. Cytologic diagnosis of adenocarcinoma was rendered. Subsequent workup with cervical biopsy was performed. The histologic features displayed nest or rosette formation of tumor cells. Foci of necrosis were also noted. Tumor cells had modest to abundant amount of eosinophilic cytoplasm with indistinctive cell border. The nuclei of neoplastic cells were large with prominent nucleoli and focal nuclear molding [Figure 2a and b]. Mitotic figures were frequent with more than 10 per 10 high-power fields. Immunohistochemical stains exhibited positive reactivity for synaptophysin, chromogranin, and CD56 [Figure 2c and d]. The expression of carcinoembryogenic antigen and p63 was not found. Based on these findings, the tumor was diagnosed as LCNEC of the uterine cervix. Thinprep cytology slide initially read as adenocarcinoma was reviewed again. Tumor cell clusters showed blurred or abortive rosettes [Figure 3a]. The nuclei were more monomorphic and round to ovoid with finely granular chromatin. The nuclear membrane was thinner than that of adenocarcinoma cells. Additional slide was made from reserved ThinPrep Pap smear vial. The synaptophysin immunostain demonstrated positive reactivity in tumor cells [Figure 3b]. Human papillomavirus typing by polymerase chain reaction was positive for HPV-16. Following the diagnosis, the patient received combined chemotherapy and radiotherapy. No metastasis or recurrence has yet been identified
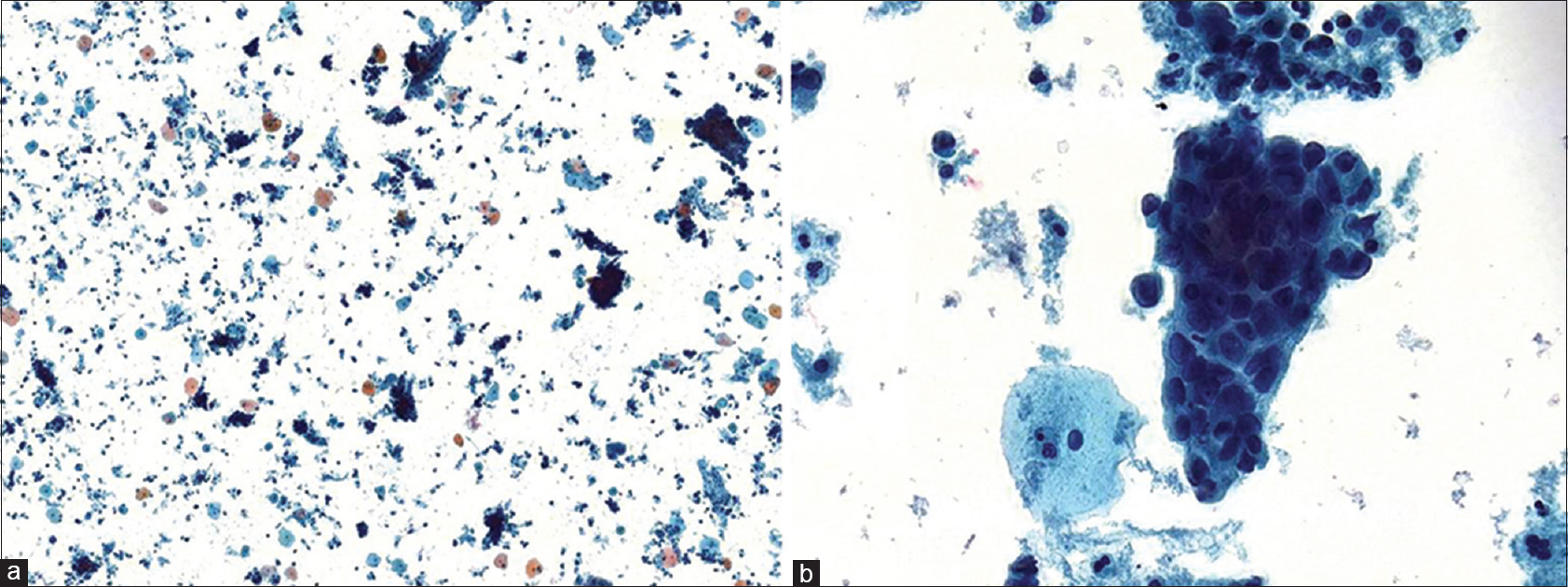
- (a) The smear shows many ball-like clusters in a necrotic background (Papanicolaou, ×20). (b) Tumor cells have large nuclei with prominent nucleoli, and moderate amount of cytoplasm. (Papanicolaou, ×400).
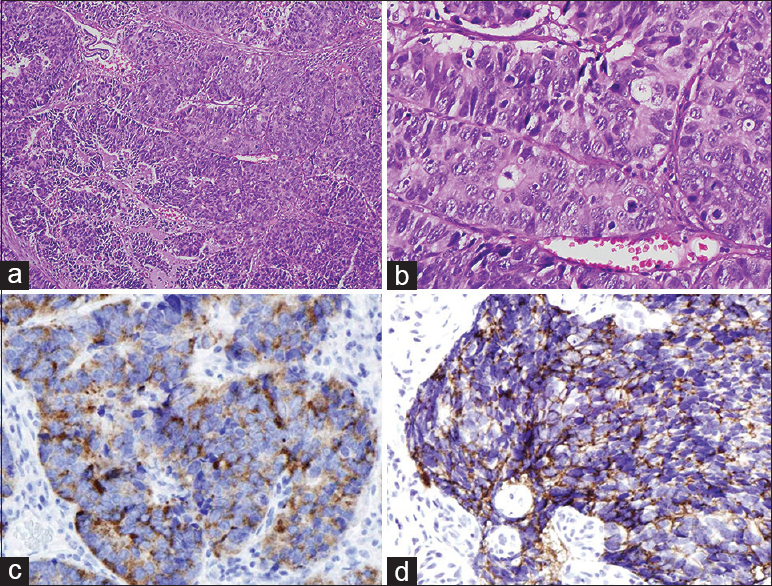
- (a) The cervical biopsy specimen shows well-defined nests, tubules, rosettes and peripheral palisading pattern of tumor cells. (b) The tumor cells have abundant cytoplasm, large nuclei, prominent nucleoli, and focal nuclear molding (H and E, ×400). (c) The tumor cells show an immunoreactivity for synaptophysin (×100). (d) The tumor cells show an immunoreactivity for CD56 (×100).
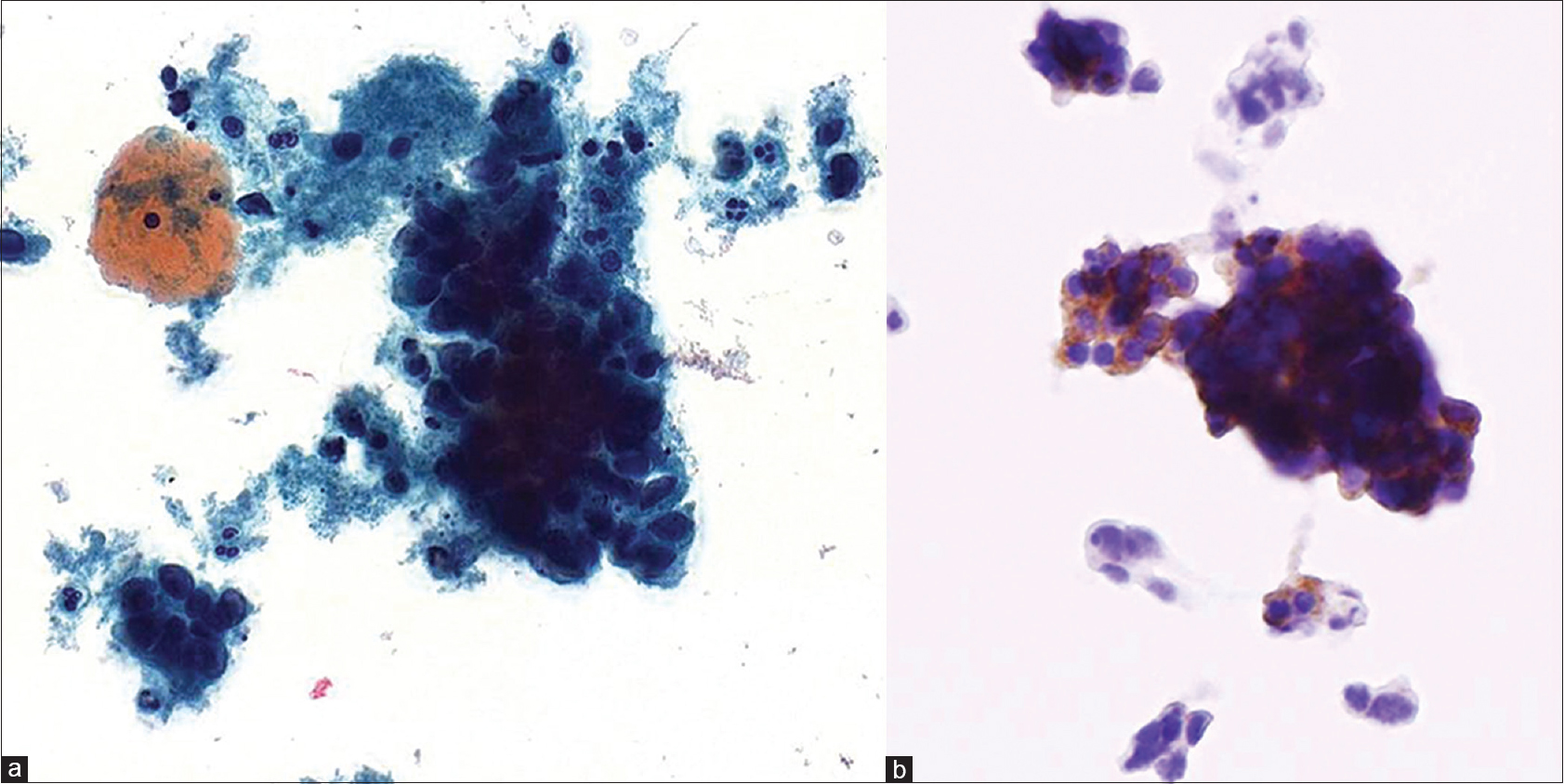
- (a) Blurred or abortive rosettes is observed in some cluster (Papanicolaou, ×400). (b) In immunocytochemistry, the tumor cells show a positivity for synaptophysin (×200).
DISCUSSION
Histologically, LCNEC of the cervix shows organoid, solid-sheet, trabecular growth patterns or rosette formation. Large neoplastic cells display moderate to abundant cytoplasm, vesicular nuclei and conspicuous nuclei. Areas of geographic necrosis are commonly seen and the tumor exhibits high mitotic rate.[6789] Unlike histologic features, the cytologic features of cervical LCNEC have not been clearly characterized.
Previously reported cytologic samples of cervical LCNEC are almost conventional PAP smears.[2345] The conventional cervical specimens demonstrated rosettoid or pseudoglandular clusters of large cells with occasional single tumor cells in necrotic background. The diameter of nuclei was three to five times larger than that of mature lymphocytes. Nuclei were ovoid with fine chromatin and prominent nucleoli were noted. The cytoplasm of tumor cells was modest to abundant. Although these cytologic findings of cervical LCNEC are similar to its histologic features, previously reported cases were misdiagnosed as high-grade squamous intraepithelial lesion, squamous cell carcinoma, and adenocarcinoma in cervical smear cytology.[2345]
In cytologic features of lung cancer, LCNEC can be distinguished from other carcinomas such as adenocarcinoma, squamous cell carcinoma and small cell carcinoma by nuclear molding, rosette formation and absence of thick nuclear membrane.[1011] Nuclear molding was observed in both conventional and liquid-based cytologic smears, but the rosettoid pattern was easily disregarded in liquid-based cytologic smears. Since it is difficult to maintain the pattern of tumor cells in liquid-based cytologic smears, there is a limit to accurate diagnosis. In addition, there are only few reported cases of liquid-based cytology of cervical LCNEC,[12] making it more difficult to diagnose.
Additional slide obtained from the remaining material of ThinPrep Pap smear vial, tumor cells showed positive reactivity of synaptophysin in immunocytochemistry. When familiar with the cytologic findings of LCNEC in cervical PAP smear, additional immunocytochemical staining must be performed to differentiate from other mimics. As the cytomorphologic features of LCNEC, its related reports increase, we believe the diagnostic criteria for the diagnosis of LCNEC will be established in the near future.
CONCLUSION
Cervical LCNEC can mislead to adenocarcinoma in liquid based cervical smear. There are many overlapping findings, such as ball-like or pseudoglandular pattern, abundant cytoplasm, and prominent nucleoli, which can be confusing, particularly in liquid-based samples. Cytopathologists should pay attention to the cytomorphologic features of cervical LCNEC, such as rosettoid pattern, nuclear molding, and thin nuclear membrane, to differentiate from other mimics. Early cytologic detection is very important in determining treatment options to improve the patient's survival rate.
COMPETING INTERESTS STATEMENT BY ALL AUTHORS
The authors declare that they have no competing interests
AUTHORSHIP STATEMENT BY ALL AUTHORS
Chang-Soo Park: Contributions to design.
Ga-Eon Kim, Nah-Ihm Kim: Acquisition of data.
Jong-Hee Nam, Jongin Na: Drafting the article or revising it critically for important intellectual content.
Yoo-Duk Choi: Final approval of the version.
ETHICS STATEMENT BY ALL AUTHORS
As this is case report without identifiers, our institution does not require approval from institutional Review Board (IRB).
LIST OF ABBREVIATIONS (In alphabetic order)
LCNEC - Large cell neuroendocrine carcinoma
MRI - Magnetic resonance imaging
PAP - Papanicolaou.
EDITORIAL/PEER-REVIEW STATEMENT
To ensure the integrity and highest quality of CytoJournal publications, the review process of this manuscript was conducted under a double-blind model. (authors are blinded for reviewers and vice versa) through automatic online system
REFERENCES
- Spectrum of neuroendocrine carcinomas of the uterine cervix, including histopathologic features, terminology, immunohistochemical profile, and clinical outcomes in a series of 50 cases from a single institution in India. Ann Diagn Pathol. 2013;17:1-9.
- [Google Scholar]
- Twelve cases of neuroendocrine carcinomas of the uterine cervix: Cytology, histopathology and discussion of their histogenesis. Acta Cytol. 2013;57:54-60.
- [Google Scholar]
- Exfoliative cytology of large cell neuroendocrine carcinoma of the uterine cervix. Acta Cytol. 2002;46:1176-9.
- [Google Scholar]
- Cervical large cell neuroendocrine carcinoma with cytologic presentation: A case report. Acta Cytol. 2010;54:977-80.
- [Google Scholar]
- Smear cytology findings of large cell neuroendocrine carcinoma of the uterine cervix. Diagn Cytopathol. 2013;41:636-9.
- [Google Scholar]
- Large cell neuroendocrine [corrected] carcinoma of the uterine cervix: A clinicopathologic study of 12 cases. Am J Surg Pathol. 1997;21:905-14.
- [Google Scholar]
- Large cell neuroendocrine carcinoma of the uterine cervix: A clinicopathological study of six cases. Int J Gynecol Pathol. 2003;22:226-30.
- [Google Scholar]
- Large cell neuroendocrine cervical carcinoma: A report of two cases and review of the literature. Gynecol Oncol. 2001;82:187-91.
- [Google Scholar]
- Diagnostic findings of bronchial brush cytology for pulmonary large cell neuroendocrine carcinomas: Comparison with poorly differentiated adenocarcinomas, squamous cell carcinomas, and small cell carcinomas. Cancer. 2003;99:247-54.
- [Google Scholar]
- Fine-needle aspiration cytology of large cell neuroendocrine carcinoma of the lung: A cytohistologic correlation study of 11 cases. Cancer. 2008;114:180-6.
- [Google Scholar]




